
ACIP meeting: Additional Pfizer dose
ACIP meeting: Additional Pfizer dose

Okay, it’s final. Phew. And I promise I didn’t leave early.
It’s recommended that you get a third Pfizer dose if you’re in one of the following groups:
65+ years
Long term care residents
50-64 years with underlying condition
18-49 years with underlying conditions are recommended to weigh their individual benefits with risks
Three important notes:
This does not include occupations (like healthcare workers or teachers). Don’t kill the messenger.
The definition of “fully vaccinated” did not change for mandates. So, if you have two doses of Moderna/Pfizer or 1 dose of J&J you are still considered fully vaccinated. You do not need an additional dose for mandates.
This is a third dose for the Pfizer series. This is not a recommendation for an additional shot for the Moderna series or J&J.
How did we get to this decision?
As a reminder, VRBPAC had a discussion last week discussing the safety and effectiveness of a third Pfizer dose. The FDA supported that vote last night. Then the ball was thrown to ACIP to make a policy recommendation.
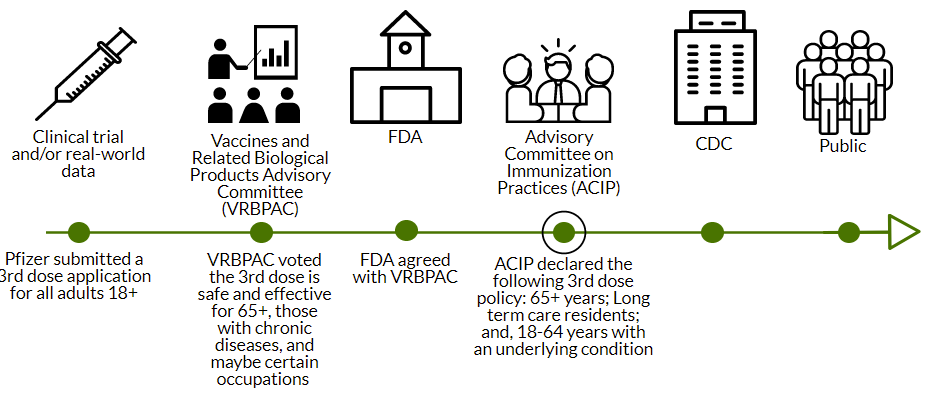
For the past two days, ACIP met to decide the policy around a third Pfizer vaccine. Yesterday’s meeting mainly comprised of the same conversation as VRBPAC (i.e. frustration around no data). But today’s meeting was incredibly informative. Importantly, ACIP needed to answer two questions:
What is the risk benefit ratio of getting a third dose?
Who should get a third dose (age, high risk conditions, occupation, and setting)?
Risk-Benefit Ratio
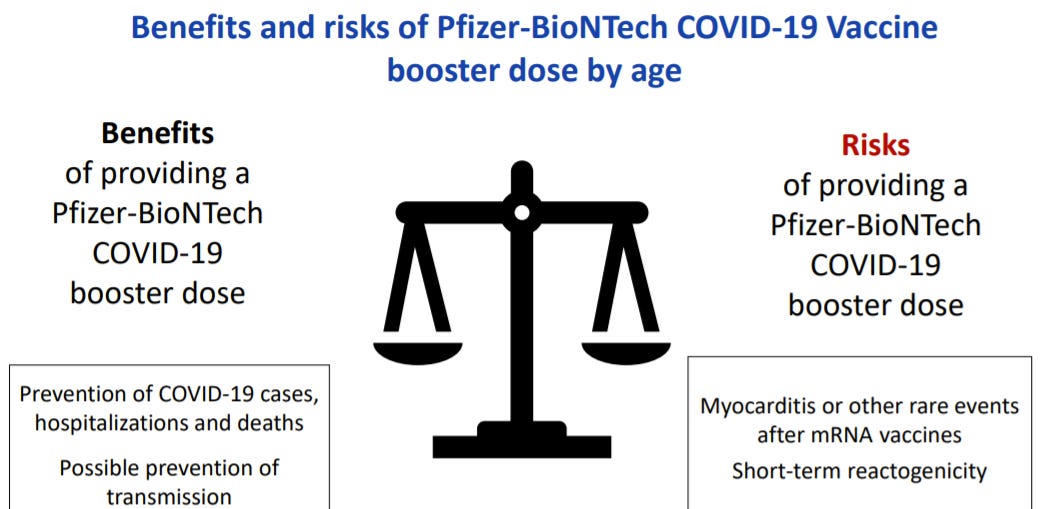
ACIP is just incredible at doing risk/benefit analyses. And today’s presentation didn’t disappoint. The question they needed to answer was: Would benefits of a third dose (prevented cases, hospitalizations, deaths, and transmission) outweigh the risks (vaccine-induced myocarditis and short-term side effects)?
They did this by assessing benefits and risks per every 1 million of additional shots administered.
For every 1 million doses, we would prevent between 7500-10000 COVID19 cases dependent on age. More infections would be prevented than myocarditis events expected. The most benefit would be for the younger population.
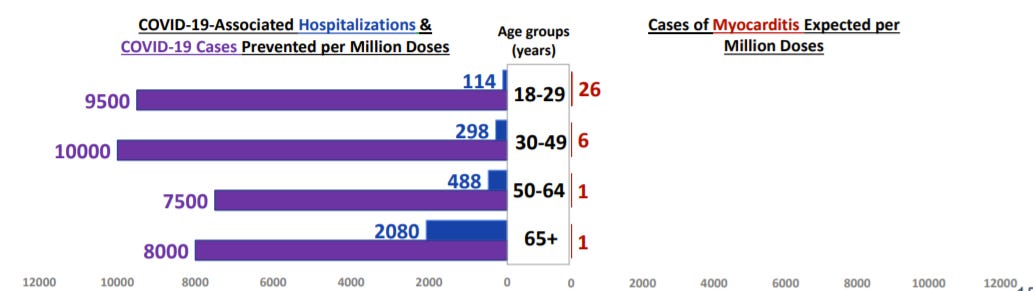
For every 1 million doses, more COVID19 hospitalizations would be prevented than myocarditis events expected. This is true for males and females across all age groups. The most benefit would be for the older populations.
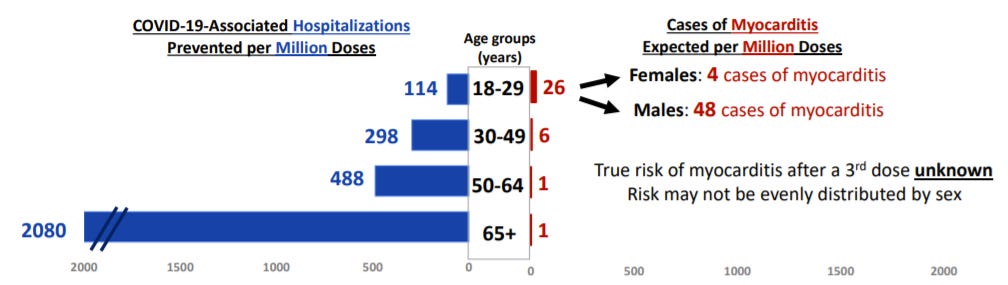
There was no discussion about reduced transmission benefit, because CDC does not have the data on this. There was also no discussion about COVID19 induced myocarditis or long COVID19 (compared to vaccine-induced myocarditis), which was disappointing to me.
Who should get a third dose?
All the voting members largely agreed that 65+ and long term care facility residents should get a third dose. There was much more discussion about age, occupation, and high risk conditions:
On one end, voting members wanted people between 50-65 years included. One voting member brought up equity. For example, American Indians, on average, don’t make it to 65 years because they are high risk under 65 years. And there is little-to-no risk of myocarditis. Others pointed that data doesn’t show (right now) that those under 65 years need an additional dose.
There was a lot of discussion about high risk conditions. For example, pregnant people with a chronic disease. Others pointed that data doesn’t show (right now) that those with high risk conditions need an additional dose.
Voting members brought up that it’s clear people want a 3rd dose, even if there’s no data yet that it’s necessary. So why not let individuals who feel at increased risk make the decision for themselves?
There was a lot of discussion about occupation and setting too. Several voting members advocated for an additional dose for healthcare workers. We could protect them from long COVID19. We could reduce absenteeism from work. We could help protect their families from transmission. After 19 months, they deserve at least that. Others mentioned that healthcare workers wear PPE and don’t get infected at work, but rather get infected in the community, so this policy isn’t helpful (I didn’t really understand this point). Similarly, some pointed out that healthy caregivers of immunocompromised kids should get a third dose so we “cocoon” the most vulnerable. But others said there’s no data on how much the 3rd dose would reduce transmission. We hypothesize this is the case, but no one has seen the data. One voting member pointed out: “We vaccinate to protect ourselves; not others”.
Vote
ACIP decided the easiest way to determine the policy would be in four separate votes. Who should get a third dose of Pfizer?
65+ and long term care facility residents: 15 YES; 0 NO
50-64 years old with underlying conditions: 13 YES; 2 NO
Individual benefit and risk (i.e. shared decision making) who are aged 18-49 years with underlying conditions: 9 YES; 6 NO
High risk occupation or setting: 6 YES; 9 NO
Bottom Line: A third dose will only move the pandemic needle a little. We need to get unvaccinated people vaccinated to end this thing. But, with a third dose, some will now be able to better protect themselves and those around them. I know a lot of people (including myself) are disappointed and angry about the occupation/setting vote. Remember this isn’t the end. There may be another vote in the coming weeks.
Love, YLE
I've been trying to find what is considered "underlying conditions". Is it still the same for those at risk for severe COVID as before? For example, high blood pressure, diabetes, obesity ( a large part of this country). Or is it simply some sort of immune deficiency? When we were waiting for vaccines, when they were first release, it seemed a large swath of the population was eligible once those over 65 vaccinated. Thanks.
Most of the teachers here have already been vaccinated for over 6 months. They need 3rd shots so there are fewer cases at schools where there are children who cant yet be vaccinated!!