



JJ will be available again, to everyone, in the US
Here are your cliff notes behind that decision

Background: Last week, ACIP had an emergency meeting to discuss the risks of blood clots (and specifically CVST + thrombosis). At the conclusion of that meeting, the committee agreed that more information was needed to make a decision regarding JJ distribution in the United States. To read more about the April 14 meeting, see my cliff notes here.
Today, the Advisory Committee on Immunization Practices (ACIP) had a follow-up meeting to make a decision regarding Johnson and Johnson (J&J) distribution in the U.S. We needed three key questions answered:
Why are we seeing these rare (but severe) cases in the U.S.?
Were there other cases during this pause?
Do benefits outweigh the risks?
Why are we seeing these rare (but severe) cases in the U.S.?
Biological plausibility (i.e. how is it physically possible that the vaccine could cause these events) is KEY to determining causality in epidemiology. So, answering this question is important.
However, during the meeting it was clear that we still don’t know how this vaccine is causing these cases. Our understanding is a moving target because cases are still popping up and all cases are not uniform with clinical presentation. We need more people to get this in order to see patterns.
But, we have a good guess thanks to the life work of a superstar scientist in Northern Germany (Dr. Greifswald):
JJ cases are incredibly similar to AstraZeneca cases. So, this safety signal seems to be due to the adenovirus biotechnology.
It seems to be an autoimmune reaction. Basically the body recognizes this vaccine as an intruder, and goes wild. We see a similar reaction among some people that get heparin (in the general population).
We don’t know why some people have this autoimmune reaction compared to other people. There are no obvious patterns yet.
Were there other cases during this pause?
Yes. We are now at a case count of 15 (out of 3.23 million doses administered to women) after clinical trials. Here are the rates for each age group

Do the benefits outweigh the risks?
The CDC compared the rate of CVST + thrombosis to the…
Background rate: 0.7-1.6 per million people
Rate among COVID patients: Extremely rare (CDC didn’t even give an estimate because it was so low)
Rate in EU (after AstraZeneca): 10 cases per million
Then the CDC ran some projections…
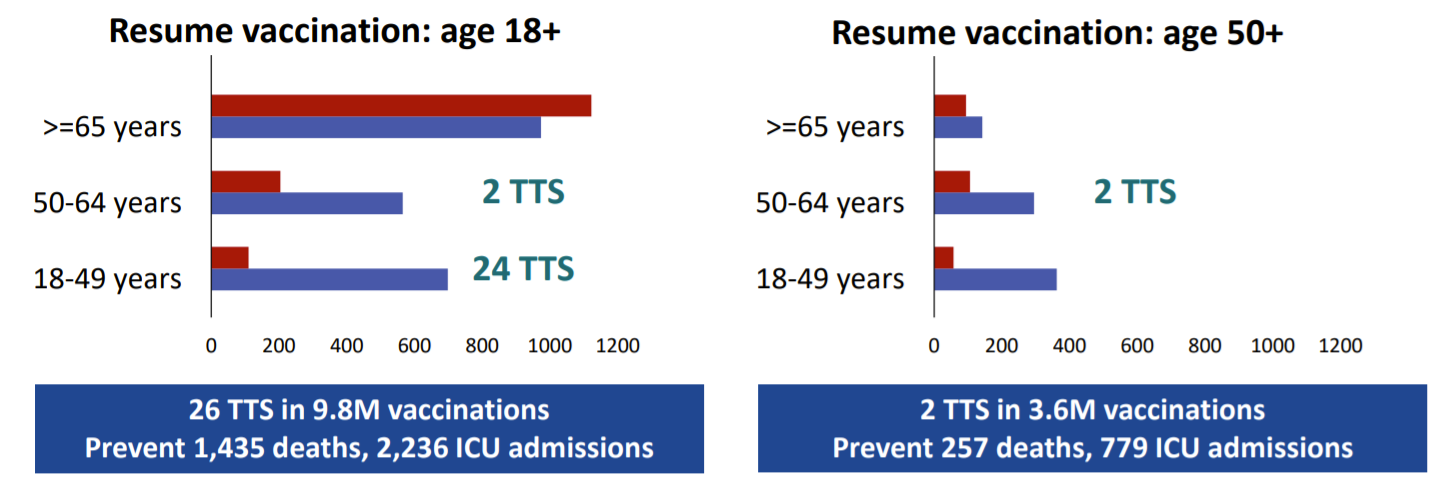
What happens if JJ vaccination resumes tomorrow for all adults (compared to stopping JJ altogether)?
Harm: 26-45 more cases
Benefit: Avert 1,435 deaths and 2,236 ICU admissions
What happens if JJ vaccination resumes tomorrow in adults aged 50+ years only (compared to stopped JJ altogether)?
Harm: 2-3 more cases
Benefit: Avert 257 deaths and 779 ICU admissions
Another big benefit of JJ?
The ability to use this vaccine to populations at risk not coming back for a second shot. For example, people in the rural population, people that are homebound, or transient populations (migrant or seasonal population, homeless, incarcerated).
Vote
So, the committee had to make a decision:
Recommend against use against all people
Recommend for all people (but put a warning on the FDA label)
Recommend for only people over the age of 50
Reaffirm recommendations for use; Women aged <50 years should be aware of the increased risk of TTS, and may choose another COVID-19 vaccine
A really interesting discussion ensued.
Many shied away from #3 because of the confusion it would ensure and logistics challenges for health departments and pharmacies. For example, places would have to stock two types of vaccines at one time, when that isn’t sometimes possible.
Some questioned why #3 didn’t include sex (women). The CDC pointed to the young male case in the clinical trial. Males have lower risk than females, but risk is not zero.
Some questioned the difference between #2 and #4. Some said that #4 would show people that ACIP recognizes the risk to women compared to #2. Wording for #4 is confusing, though, and can seem shady (which would fuel misinformation).
The group ultimately picked #2.
Have a great weekend.
YLE