



Confused about the 3rd dose? Me too

Today the White House COVID19 Task Force announced their support of a 3rd dose for the mRNA series among the general public. Starting September 20 (and assuming that the FDA and CDC agree), people can get their third dose 8 months after their second dose.
This has been a rollercoaster to follow
It’s been a confusing story as there’s a lot of rapidly moving parts. We’re watching the scientific process unfold in real time, which is actually quite beautiful. Science is not static. Our understanding changes and morphs with more and more evidence. If it doesn’t, then scientists are not doing their job. The virus also continues to mutate, so the science has to continue to re-evaluate.
Concurrently, we’re watching how science then informs policy. Usually this is done slowly (unfortunately with public health), but the institutions are acting fast to the ever evolving landscape of the pandemic.
Nonetheless, it’s confusing. Even for me. So, here is a recap of what’s happened in the past 2 months regarding a third dose for the general public. I organized this Figure to distinguish what’s happening from the science and institution/policymaking perspective:

So, this is where we are at…
Vaccines continue to protect against severe disease and death
This is clear. And we are incredibly lucky this is still the case. There have been many studies confirming this around the world. Today, two additional studies from the CDC were released to add to this evidence base.
The first study, using data from New Yorkers, found that from May 3–July 25 vaccine effectiveness against hospitalization was stable over time (ranging from 91.9% to 95.3%).
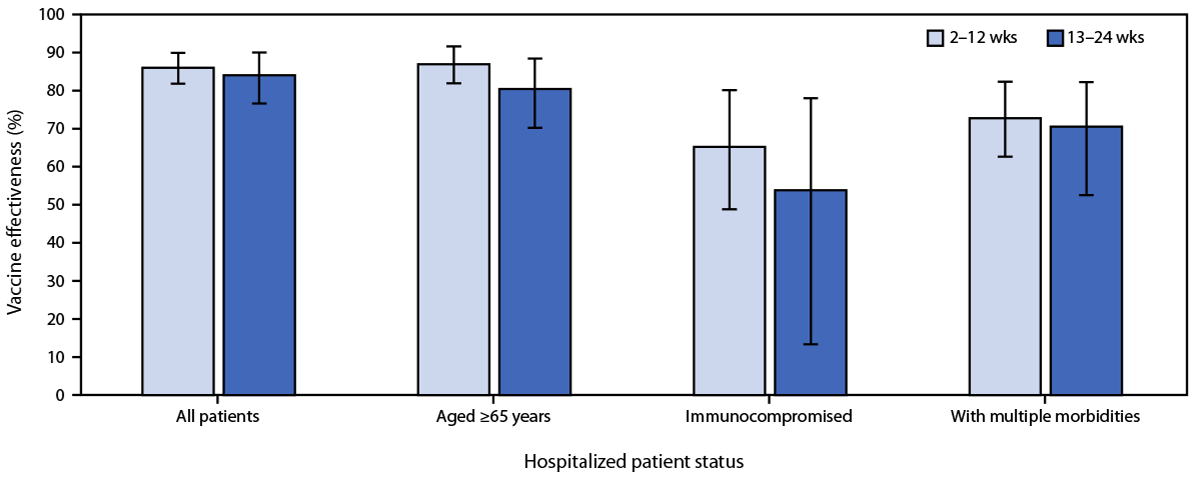
The second study looked at hospitalizations at 21 medical centers across 18 states over a 24 week period (March to July 2021). The scientists found no decline in vaccine effectiveness against COVID-19 hospitalization. Vaccine efficacy didn’t change based on time of vaccination: Vaccine effectiveness was 86% 2–12 weeks after vaccination and 84% at 13–24 weeks. It also didn’t matter whether you were “high risk” (65+, immunocompromised, or multiple comorbidities; see figure below).
The question is efficacy against mild to moderate disease
The real question is how do the vaccines protect against asymptomatic, mild and moderate disease. Thankfully, Israel and the UK have public health infrastructures to evaluate these numbers in real time. While the data from the two countries disagree on the exact efficacy number (probably because of reasons I posted here) it’s clear that it is reduced.
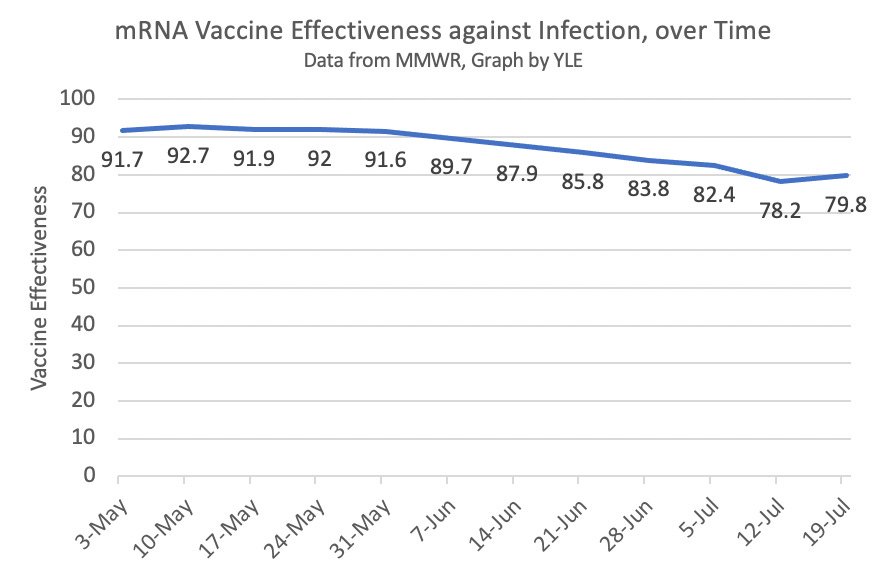
This week we confirmed the international data with national data from three important studies. The first study used data from Minnesota Mayo Clinic. They found that efficacy was reduced in July compared to earlier months. A second study from the CDC was released today using data among New Yorkers. From May 3–July 25, vaccine effectiveness against overall infection declined from 91.7% to 79.8% (see figure). The third study found this decrease was even more dramatic among nursing home residents (74.7% to 53.1%).
We don’t know if the reduced efficacy is because of Delta or because of waning immunity (antibody response getting weaker over time) or both. Slides from the White House meeting today suggested that it has to do with waning immunity (not Delta). A Moderna study found that antibodies decreased over time regardless of variant.

So, why do we need a third dose?
Boosters are not new. In fact, in order to attend kindergarten, kids need five D-TAP shots, four polio shots, two MMR shots, three Hep A shots, and two chickenpox shots. HPV needs a booster after a year. Tetanus needs a booster after 10 years.
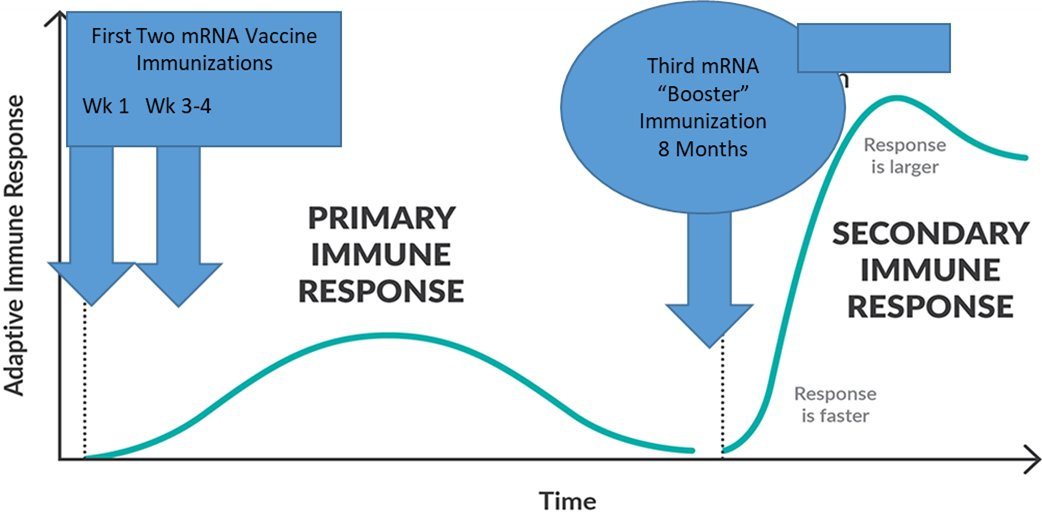
Some, like Dr. Hotez (a brilliant immunologist), have said a COVID19 third shot was inevitable because our two doses were too close together. Booster shots are most effective if they are at least 6 months apart. Back in Dec/Jan, we were losing 3,000 people a day to COVID19 disease, so we gave the full protection (2 doses) only 3-4 weeks apart knowing that we could be sacrificing durability of protection. Other countries, like the UK and Canada, decided to give their doses further apart.
A third dose has stirred quite the debate among scientists
On one hand, people think this is too soon for the general public to get a third dose. Vaccines are working beautifully against severe disease and death. Vaccine efficacy against mild and moderate is decreased, but not dramatically for the general public. Vaccine antibodies are decreasing, but we expected this. We don’t know how our well our adaptive immune system is doing (i.e. T-cells and memory B-cells). Vaccines could also be better used in other countries. Only 31% of the world is vaccinated. The next variant of concern can pop up anywhere in the world, which will then directly impact the US anyways.
On the other hand, (and the White House’s argument) is that this is a proactive approach. (I do applaud them for this as we have always played a reactive game and it’s exhausting). It takes time and effort to get another 100 million doses in arms. Vaccine efficacy against hospitalization and death could start decreasing with time (or with the next variant). Also, it looks like people are already getting their third dose regardless (about 1 million Americans have already done this), so might as well organize this in some sort of fashion.
Bottom Line
This is probably more than you ever wanted to know. A third dose is coming for you. I’m not convinced that I (a healthy, young person) needs it. I much rather give it to another person in another country. Or, hell, I rather a kid be able to get their vaccine. But I will stand in line come September if it’s recommended.
Love, YLE
P.S. Sorry J&J people… we are still waiting on data for you. Don’t kill the messenger.
I’ve been looking at the Mayo study. Am I understanding correctly that 1/6 of the “vaccinated” only received 1 dose of mRNA? Wouldn’t that skew the results when deciding if a 3rd dose is needed?
I would much rather see the rest of the world getting initial vaccines rather than boosters for the general US public. Besides the issue of fairness, won't this help reduce spread?