



Limited access to abortion is a public health issue: How you can help

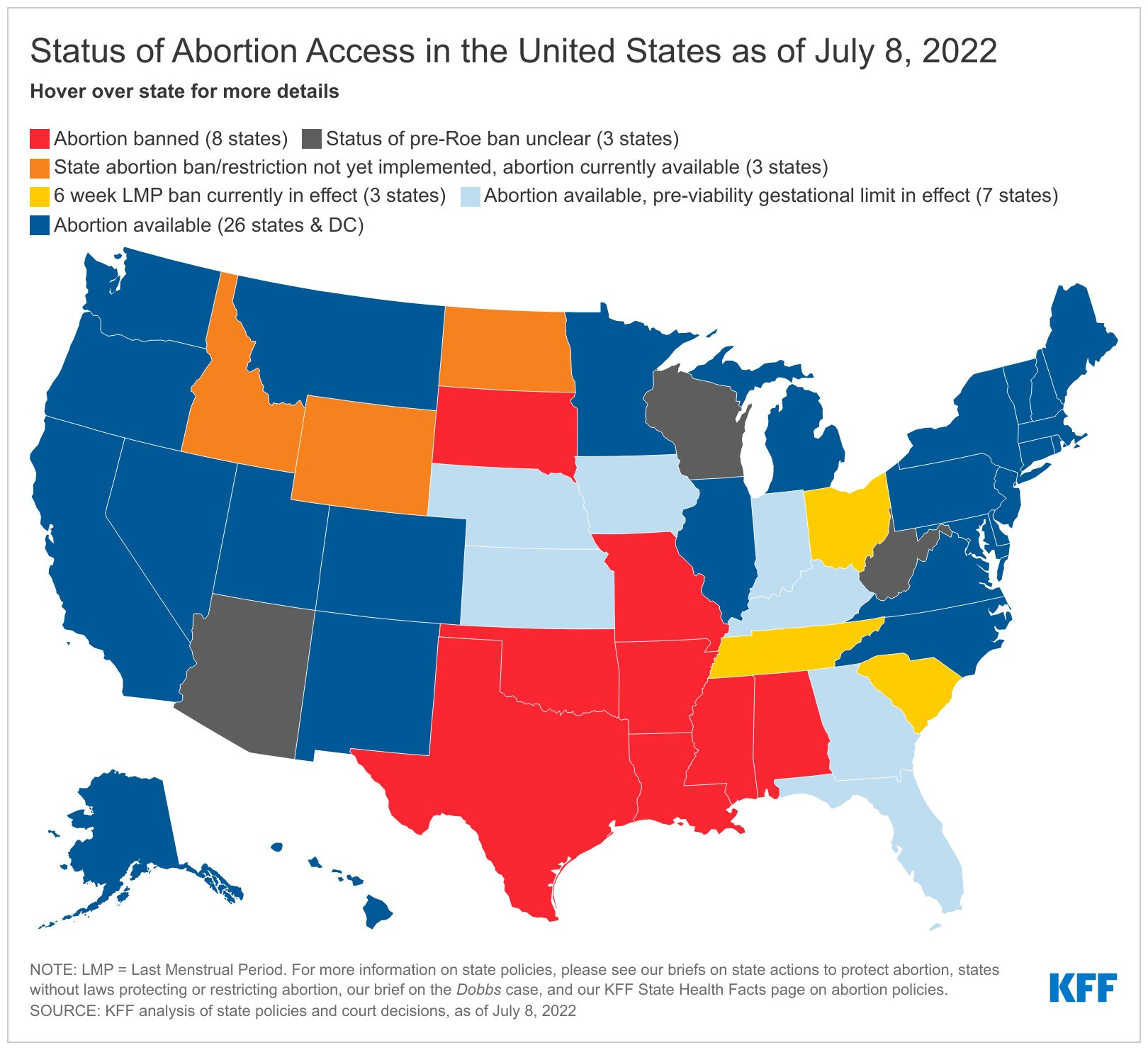
Roe vs. Wade was overturned two weeks ago. Access deserts quickly popped up, as shown in red on the Kaiser Family Foundation figure below. This will only grow with time.
Although the Biden administration announced an executive order to protect access to reproductive health care services (including IUDs, interstate travel, data privacy, and legal services), it’s not clear how much rubber will hit the road. For example, it doesn’t fund interstate travel and doesn’t direct the Department of Justice to sue states that ban abortion pills.
Severely restricting access to care will (or already does) have a direct impact on the short- and long-term health of individuals seeking abortions and our broader community. It will be a public health disaster for decades to come.
Last week, I sat down with Robin Marty to discuss access, how it affects individuals and communities, and what we can do to help right now and in the long term. Robin is the Director of Operations at an abortion clinic in Alabama and author of Handbook for a Post-Roe America: The Complete Guide to Abortion Legality, Access, and Practical Support.
Listen to our conversation here:
During our chat, multiple organizations were mentioned. Here are their direct links:
AidAccess.org (a group based in Austria that can mail the same abortion-inducing medication)
If/When/How: Lawyering for Reproductive Justice (provides a confidential legal help line and defense fund)
Donate to clinics (if possible, make recurring donation rather than one-time)
Practical support assistance: Midwest Access Coalition (getting people to care) and Elevated Access (group of pilots flying people)
Brigid Alliance (volunteers in NY who provide homes for later abortions)
Here’s how to locate your closest local abortion clinic for support (email and be patient)
Love, YLE
In case you missed it:
“Your Local Epidemiologist (YLE)” is written by Dr. Katelyn Jetelina, MPH PhD—an epidemiologist, biostatistician, wife, and mom of two little girls. During the day she works at a nonpartisan health policy think tank, and at night she writes this newsletter. Her main goal is to “translate” the ever-evolving public health science so that people will be well equipped to make evidence-based decisions. This newsletter is free thanks to the generous support of fellow YLE community members. To support the effort, please subscribe here:
Thank you. You're on the side of the angels.
Thank you for this post and your conversation with Robin Marty. One of the really important things she said, that needs to be said over and over and over, is that "6 weeks" of pregnancy - the point at which 6-week abortion bans take effect - is really just 2 weeks after the earliest a person might find out they are pregnant. I wish that journalists talking about reproductive health care and rights would more often clarify that "6 weeks" is really just 2 weeks - at most!
Another area where people really need better information, and where I bet you could help, Dr. Jetelina (and/or you might know other epidemiologists who could), is about 2nd trimester abortions (and even the very rare 3rd trimester ones). Information about numbers of 2nd trimester abortions and the reasons for having an abortion then rather than earlier needs to be widely shared and clarified. Due to a lack of information, (and plenty of other factors), people have misconceptions that lead them to say things like that they support restrictions on "late-term" abortion, or on abortion past the 1st trimester. How many 2nd trimester or later abortions are happening because people couldn't get access earlier? What were the barriers to access? How many are due to medical reasons that weren't known until the 2nd trimester?
I was also really glad to hear her remind us that in addition to all the other reasons it is a problem for people who need an abortion to need to travel long distances to get that care, that there is also the increased risk of covid to consider if someone has to travel!