



Mu vs. Delta. Does it call for a Delta booster?

Thanks to all 57,262 (!!) of you that have already completed the “Who are you?” survey. I know there were a few times we broke Google because of high traffic. So, if you are one of those people who couldn’t get in or was told they were a robot… the problem seems to be accessing the link directly from Substack/FB. If you have the patience for one more time, try copying and pasting the survey link in your browser. And, for those of you that don’t know what I’m talking about… please take this short survey about YLE's audience and future. It’s 20 questions with a few pages, so be sure to click through. I hope to share the aggregate results with you soon. Thank you!!
Here is the survey: https://forms.gle/dgu4KEg5VUwC9yaV6
Mu vs. Delta: An Update
Last month I covered Mu— a new SARS-CoV-2 variant the World Health Organization announced as a “Variant of Interest”.
Briefly, Mu was first discovered in Colombia in January 2021. It since spread across the globe, including the United States. There was considerable interest in this variant because, as the WHO stated, it has a “constellation of mutations that indicate potential properties of immune escape”. In other words, there are number of changes on the virus in which our treatments and vaccines may not recognize, and, thus not work.
On August 31, the WHO announced it was closely watching how Mu competed with Delta in Colombia and Ecuador. Can Mu outcompete (i.e. more transmissible) Delta? Because if it can, we may be in trouble.
What has unfolded since?
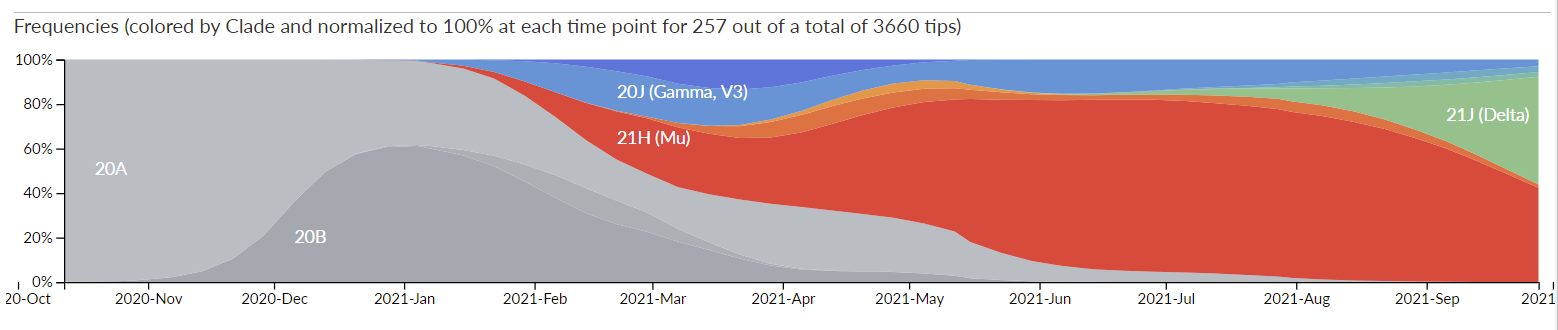
In Colombia, Mu became the dominant variant in May 2021. In June, Delta was introduced and, in recent weeks, has been slowly pushing Mu out of the way.
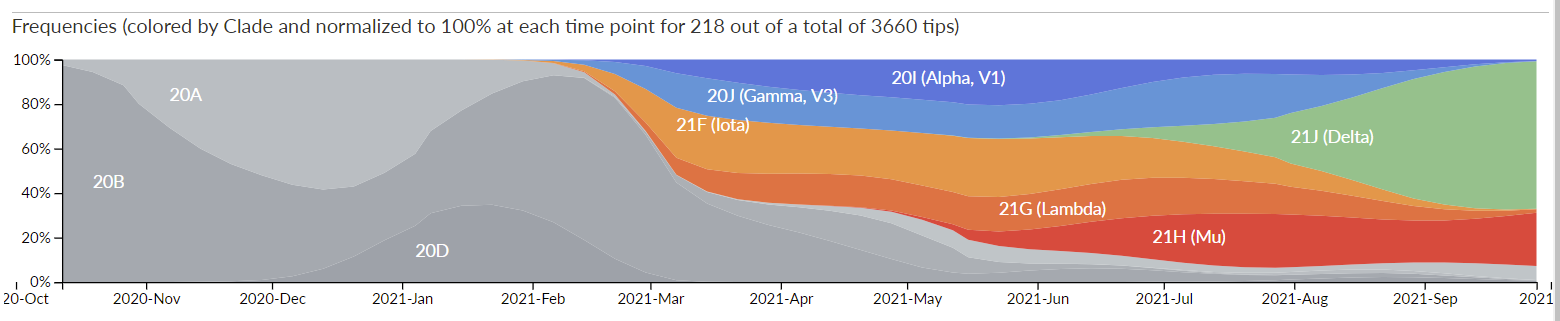
In Ecuador, Mu arrived in May 2021 and has been holding steady for the past three months. But another data source (second graph below) is showing a much different picture in Ecuador. Recently Mu started increasing and pushing Delta away. According to this data, 50% of cases in Ecuador are Mu and 50% of cases are Delta.
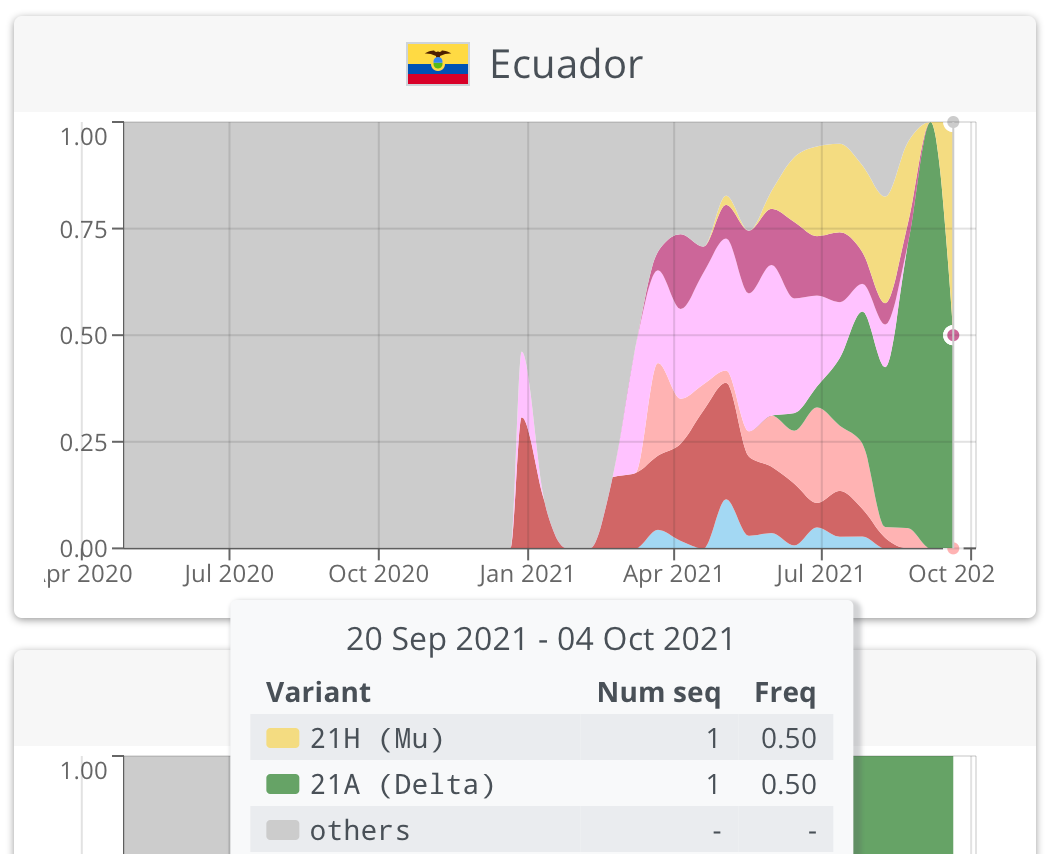
There is a significant challenge with following variant dominance in Ecuador: They have a very small genomic surveillance program. From August to September, only 12 samples were sequences (compared to the UK which sequences 10,000 per week). So we have to take uncertainly into account. When we do that, the “true” prevalence of Mu ranges from 0-60% of cases. This is a really big range, so we’ll just have to continue to see how Mu vs. Delta plays out in Ecuador.
What about the United States?
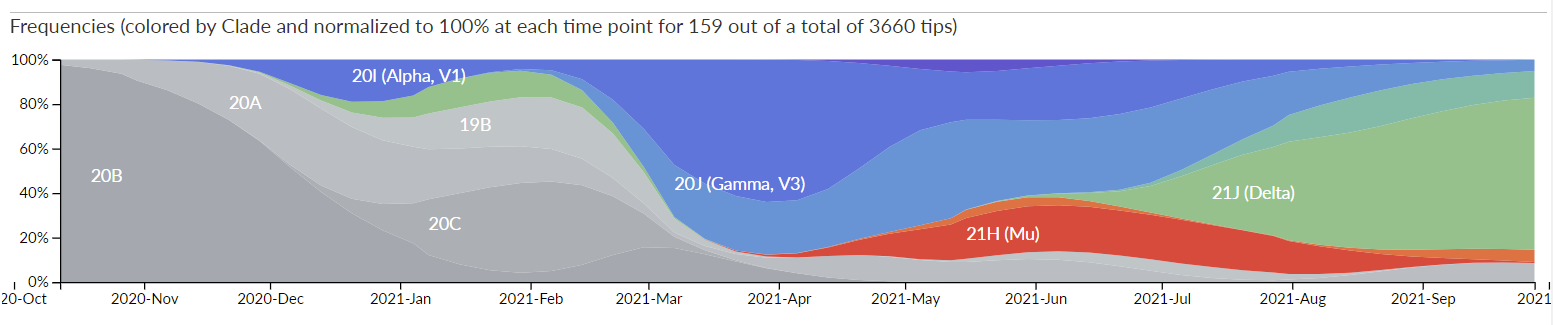
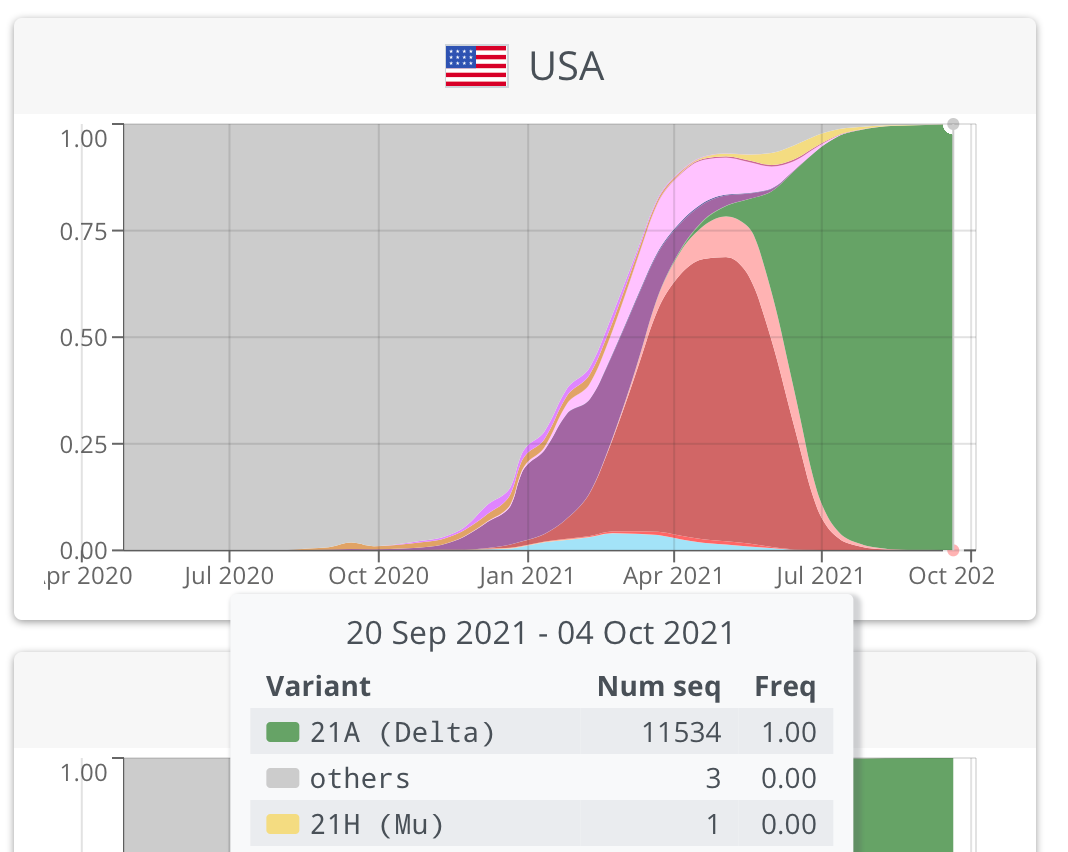
In North America, Mu was introduced in April 2021 and started spreading quickly. However, Delta came along in June 2021 and quickly became the dominant variant by August. In the United States, specifically, the CDC is now reporting zero cases of Mu. Delta accounts for 99.8% of cases.
We’re seeing this in the science too.
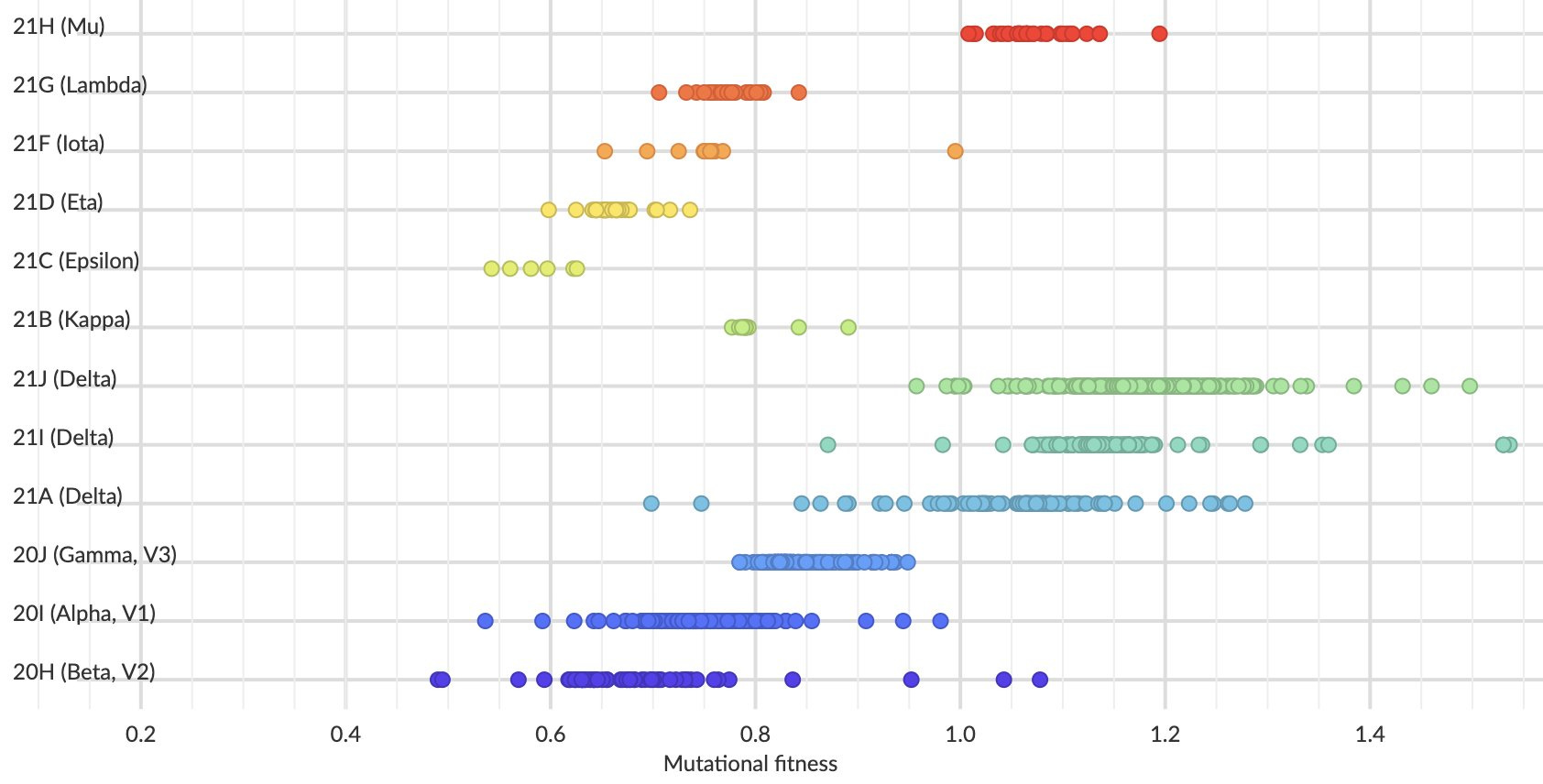
One team found Mu (red) was, on average, more fit than previous variants. Compared to Delta (green and teal), Mu is not as fit. But this is on average; there is significant overlap in our certainty (some red dots overlap with the green/teal dots).
So, Mu isn’t an immediate threat for the United States. (Thankfully?) Delta was introduced. If it wasn’t, Mu would certainly be the dominant variant right now and, possibly, escaping our vaccine and natural protection.
Going forward, we need to focus on how Delta is changing:
Is it becoming more transmissible? There is a point at which transmissibility caps out.
Is Delta mutating to eventually escape our vaccines? And, if so, how quickly? This doesn’t cap out. Viruses can change slowly over time (like Measles that doesn’t mutate at all) or fast over time (like the flu).
As Dr. Trevor Bedford (a brilliant scientist that assesses viral dynamics) said:
“So far, there is little signal [of Delta changing] but I should expect such sub-lineages to emerge in the coming months”.
Since Delta is the threat, should we wait for a Delta-specific booster?
Pfizer is testing a vaccine that specifically targets Delta. Results from the clinical trials are anticipated in the forth quarter of 2021. Moderna also announced that it’s testing a Delta vaccine (and, more interestingly, a combo vaccine that targets both Beta and Delta).
So, should we wait for a Delta booster? No. For four reasons:
We don’t know if we need them at all. There are some studies that show a third dose of the same vaccine formula is just as good as a third dose of a vaccine with an adjusted formula.
If we will need them, we certainly don’t know when. While we expect the variant to mutate, we don’t know if it will mutate enough to warrant another vaccine.
If we needed them today (which we don’t), it would still take weeks (if not months) to get the data, go through regulatory approval, and distribute the new vaccines across the country.
We do know that vaccine efficacy is suboptimal for immunocompromised. We also know that efficacy is waning. Right now. Especially for those 65+ or got the vaccine more than 6 months ago. So, if you’re in a high risk category, get the original booster formula. We need you protected now.
Love, YLE
P.S. Thanks to Dr. Bedford for the Mu reminder yesterday on Twitter! And, as always, his brilliant analyses and contribution to the field.
A couple of random thoughts. Mu and Delta were the first two variants that showed any significant change in the conformation of the spike protein that might cause problems for the "neutralizing" IgG created by the mRNA and adenovirus-vector rDNA vaccines. That was what raised the interest of the WMO. Although I should be paying more attention to international surveillance, I've got this odd limit on time, since i'm not embedded in a department or research group, so I've focused on the US, and for the most part, CONUS, looking at Alaska and Hawaii when needed...
Delta has shown us some nasty tricks. It produces more viral replication product (particles) per cycle than WHU-1 or Beta, for instance, and the minor changes in the S1 protein allow it to show more affinity for the ACE2 receptor. Mu shared some of these properties but not at the same level as Delta, hence, in my mind, its lower competitive advantage overall. Were we to solely look at the S1 conformation changes in Mu, we'd have expected its resistance to our antibodies to be a bigger advantage, but there are so many factors to consider here, sometimes the obvious fails to win.
The research I've read shows the current vaccines are adequately effective against Delta. Their efficacy against Mu would require more available virus, and clinical observation with adequate genomic testing would be simpler than an in vitro estimation of efficacy. That didn't work out.
As to whether we need a Delta-specific booster... I currently don't think so (but like so many other things in this pandemic, I might have to change my mind). At least in the US, and other countries where Delta's predominated, it's burned through the susceptible population virtually unimpeded, because so many who acquired this strain were unvaccinated, and didn't really believe in either the virus overall, or the use of NPIs for mitigation. The sharp upward trajectory, short time at peak and sharp downward trajectory are what I learned in school as the shape of a "normal" pandemic where nothing is, or can be done to mitigate its spread.
I've said earlier that I have little faith in immunity conferred by infection providing any longer, or better protection than immune response conferred by the vaccines. The "why" is that the infection-conferred immunity tends to be more specific to the variant you've contracted, and there's some serial evaluations of humeral immunity that suggest its duration is shorter than the vaccine-conferred humeral immunity. Activation and training of the cellular immune system is also interesting as there are a couple of papers suggesting that cellular immunity training and activation by naturally conferred response is much more variable than that initiated by the vaccines.
I propose this is because infection-conferred immunity has the entire spectrum of antigenic triggers from a particular strain and may in fact train IgG to look for a more complete component, where the vaccines provide triggers for fragments of proteins, which allow less-specific response, but a response more tailored to the spike and plasmid capsule of this species of coronavirus... so is likely more effective overall.
What this suggests to me, today, pending more research, and likely another wave of cases down the road, is that the current set of vaccines authorized or approved in the US today are effective as they are.
Most likely, we don't still have a lot of unvaccinated, Delta-susceptible individuals left. Part of the reason is, I'm convinced (again... as of today at 0715) that recent prior infection likely confers some protection for at least 90 and as long as 180 days against the general SARS-CoV-2 virus regardless of which variant lineage it claims. As a result, I think we're looking at 4-6 month of relative quiet, when, hopefully, all our holdouts will get vaccinated and Merck and others will get their COVID-specific antivirals out to clinical availability. And then, I expect we'll see anther wave, caused by a variant imported via air transport from a part of the world still serving as an incubator for new variants because they're inadequately vaccinated. And the public will have already told us that, to them, the pandemic's over.
My thoughts, so there's no one else to blame organizationally...
So, if the vax works better against Delta than Mu, you might expect Mu to have a fitness advantage in vaxxed folk. But, with so many people being vaxxed, the prevalence of Mu hasn't increased. Am I thinking about this correctly?