
Omicron Update: Nov 29

In an attempt to keep you up to speed, here’s an Omicron update.
1. All U.S. adults should get a booster.
Before today, this was CDC’s recommendation for boosters in the US:
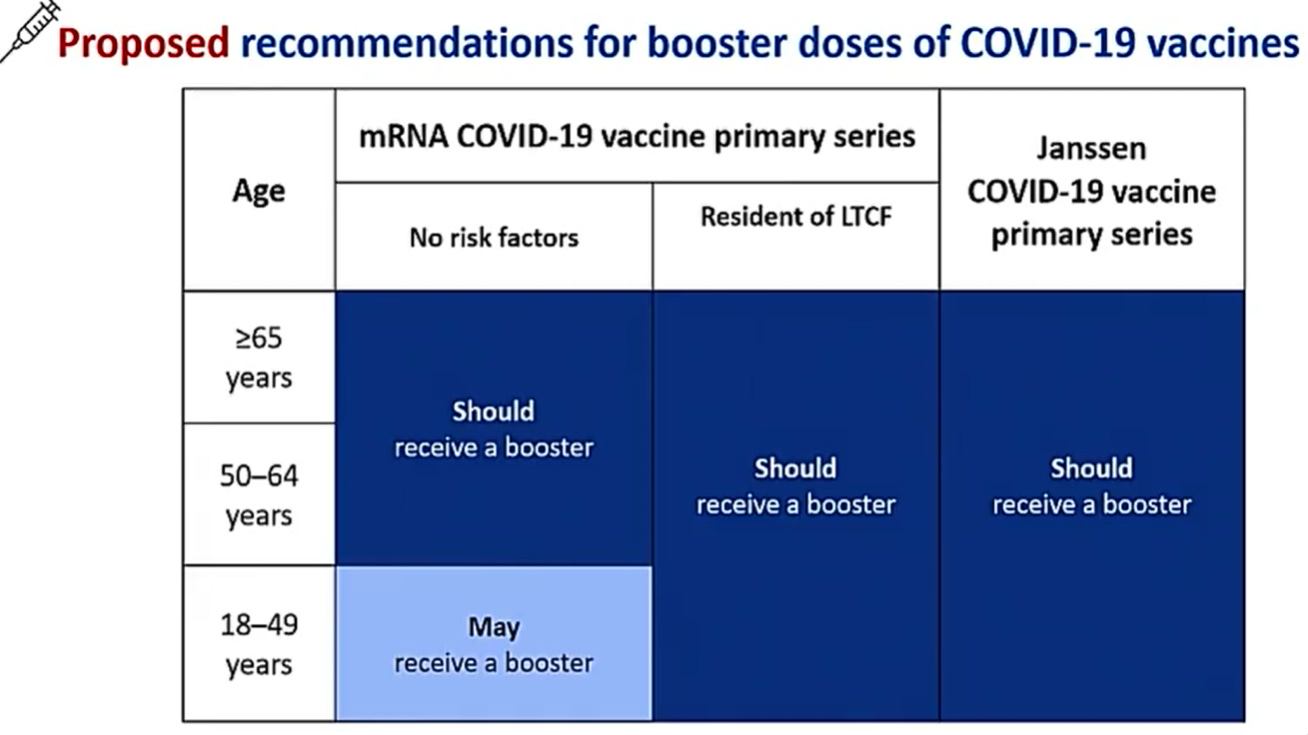
The CDC changed its recommendations today. Now, all adults should (not may) get a booster. Like I posted yesterday, we have reason to believe that boosters will help protect against Omicron. (Parents: no word yet on 12-17 year old boosters).
2. WHO Update
Last night the WHO provided an update, which basically said we still have more questions than answers: Is Omicron more transmissible? How do vaccines work against Omicron? Does Omicron cause more severe disease? We don’t know, but we’re working on it. There were a few sentences worth highlighting, though:
“Preliminary evidence suggests there may be an increased risk of reinfection with Omicron (ie, people who have previously had COVID-19 could become reinfected more easily with Omicron), as compared to other variants of concern, but information is limited.”
So, infection-induced immunity (some are calling it “natural immunity”) may not work well against Omicron. This isn’t a surprise because we saw this with Delta too: Those with infection-based immunity were 5 times more likely to be reinfected than those with vaccines. Time for the unvaccinated to get vaccinated.
3. What’s happening on the ground in South Africa?
As expected, cases are rising. Omicron has been identified in each region in South Africa, so exponential spread is well on its way. A South African epidemiologist estimated that by next week there will be 10,000 new cases per day in South Africa.

An increase in cases means Omicron is spreading. This does not necessarily mean Omicron is more transmissible (i.e. more contagious/ higher R(0)) than Delta. We have to marry lab data (what are the specific mutations doing) with “real world” data (does Omicron outcompete Delta in places with high rates of Delta, like the US) to see.
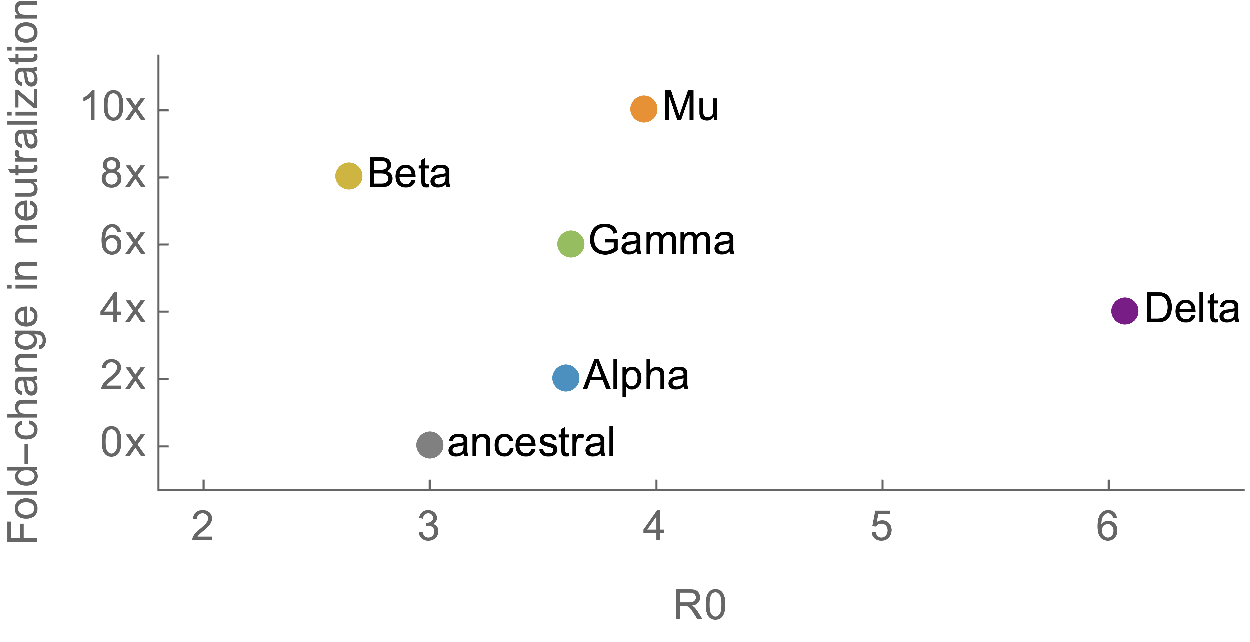
Keep in mind that there is a possibility (some say strong) that Omicron will be less transmissible than Delta. That’s because there’s a trade-off between immune escape (or immune corrosion) and transmissibility. We’ve seen that with other variants of concern. In the figure below, transmissibility (or contagiousness, or R0) is on the horizontal axis and antibody effectiveness on the vertical axis. The higher in either direction, the worse. To know where Omicron is on this chart is a complex, scientific guess at this point.
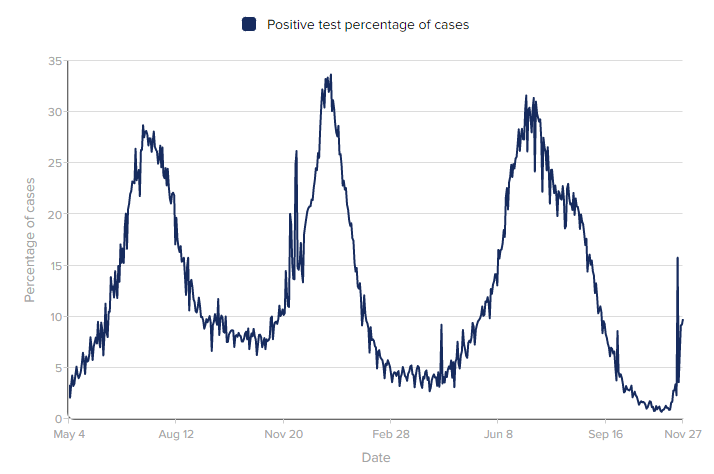
Back to South Africa... Test positivity rate (TPR) is also increasing. TPR has consistently been an early indicator of what’s to come. TPR indicates whether a community is testing enough to catch the virus. We decrease TPR by increasing testing: People learn they are positive, they isolate, and stop spreading the virus. Early in the pandemic, the World Health Organization advised countries to strive for a 5% TPR. As of November 27, TPR in South Africa is at 9.77% (3,220 cases from 34,880 tests). This is not terrible, but not great.
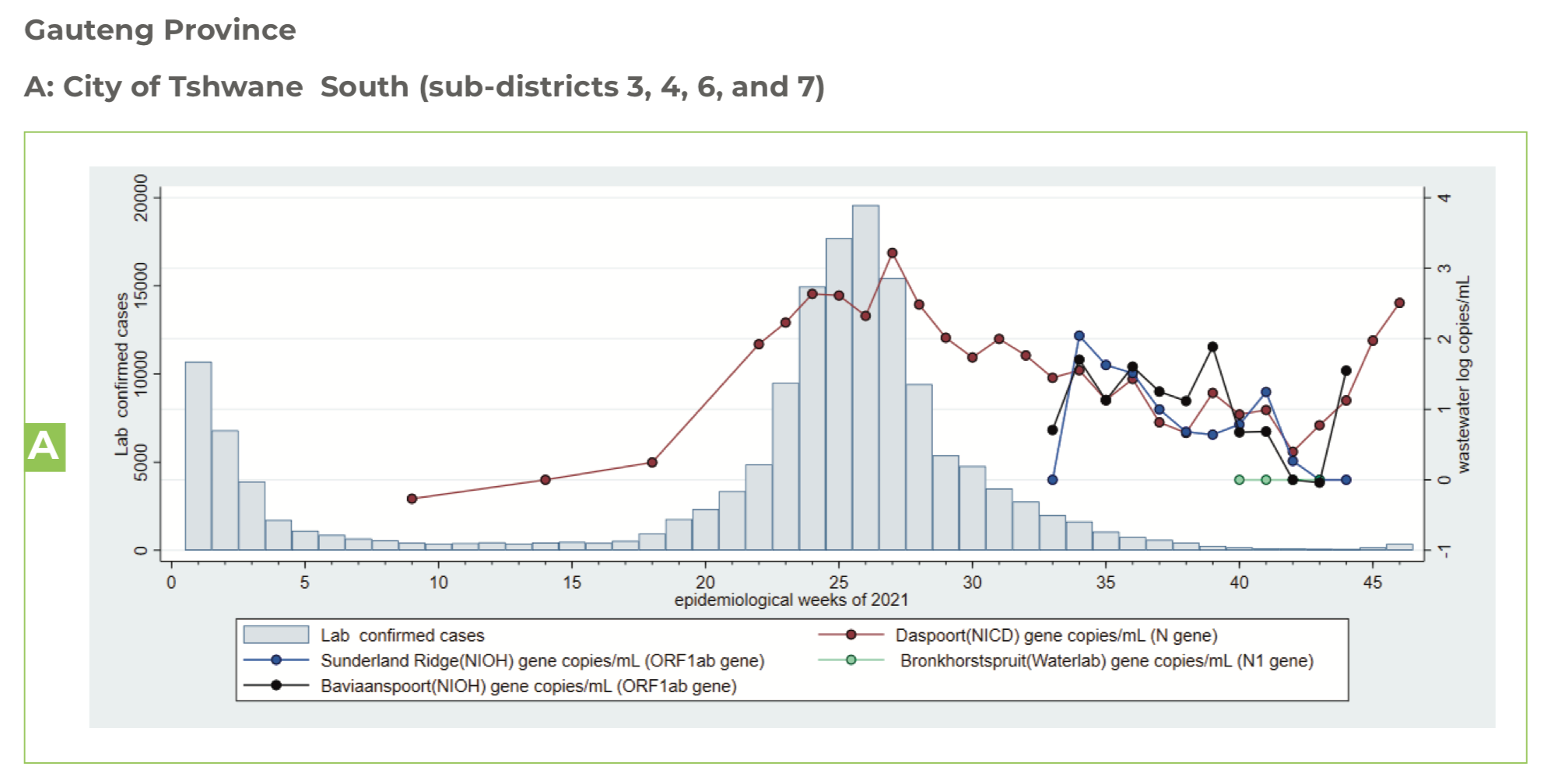
We are also seeing a rise in wastewater tests. Wastewater is actually an incredibly accurate, early indicator of case rise. The figure below shows wastewater tests in the city of Tshwane (near South African epicenter) alongside lab confirmed cases. Detection of COVID-19 in wastewater is almost as high as it was with Delta. So, this could mean a rise in cases is coming. This also could mean that cases are mild so they are going undetected. Time will tell.
On a national level, we don’t see a rise in hospitalizations in South Africa. But hospitalization trends lag case trends 2-4 weeks, so this may be coming. This pattern has been consistent throughout the pandemic.
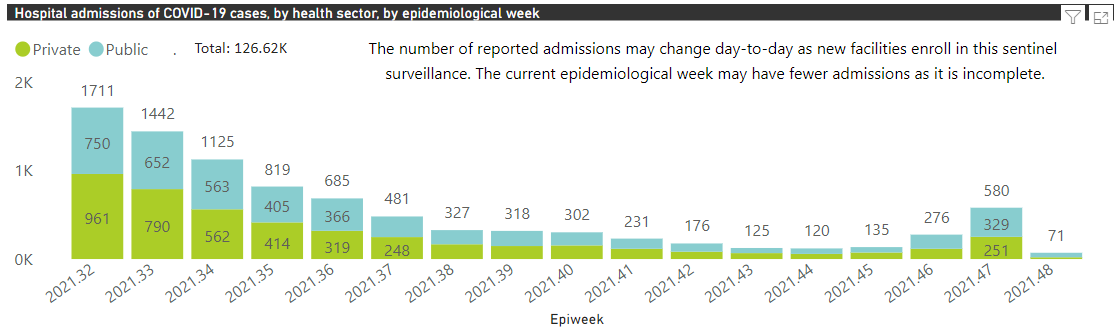
However, if we zoom in on South Africa’s epicenter— Gauteng— we start seeing a rise. Below is a graph from the National Institute for Communicable Disease. The bars are hospitalizations per week (Monday - Sunday). Last week, there were 580 COVID-19 hospitalizations, which is a 110% increase from the previous week. This week just started, and there are 71 hospitalizations so far.
It’s important to note that this increase in hospitalizations isn’t necessarily because Omicron is more severe than other variants. It could just reflect the fact that more people are getting infected. Parsing this out is key to understanding Omicron.
In the past 24 hours, there’s been news about “mild presentation” of Omicron, leading some to the conclusion that that Omicron is not severe. I sure hope this is the case, but be cautiously optimistic. Those were only ~100 mild cases among young people and do not represent country-level demographics.
4. What’s happening in other parts of the world?
As expected cases are starting to pop up all around the world— 5 continents, 21 countries, and 195 confirmed cases. At some point there’s no point to tracking this, but for now it’s fascinating for epidemiologists to follow.

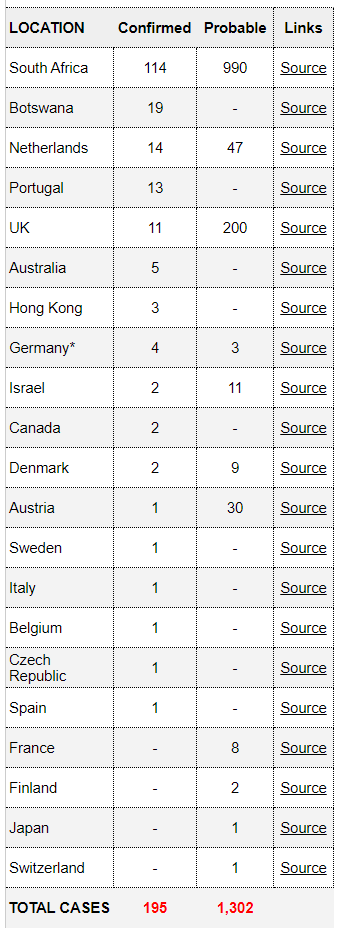
When you hear about cases in the news, it’s important to distinguish whether these cases are from travel or from the community. If a case has no travel history or no contact with someone who has traveled to South Africa (like the 3 cases in Israel), this is a clue that Omicron has already been spreading.
5. Why haven’t we found a case in the United States?
We hypothesize that Omicron is already in the States; it’s just been flying under the radar. We don’t have a confirmed case yet.
Our genomic surveillance system is suboptimal given our large population. While it’s getting better, it’s ranked 20th in the world.
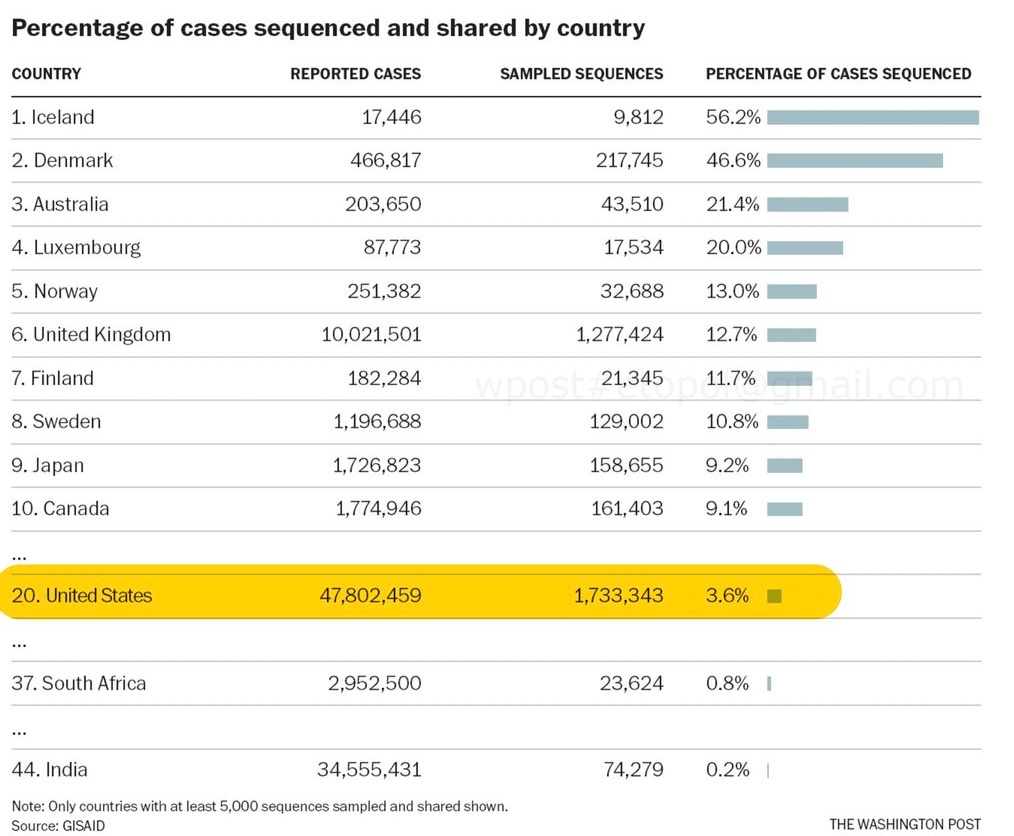
Regardless, we have 68 Public Health Labs sequencing 15,000-20,000 specimens to search for variants like Omicron. We also have commercial labs, CDC contract labs, and academic labs. Nationally, ~5% of all specimens are sequenced. This means our system can detect down to 0.01% of circulating variants. So, Omicron can be found…eventually.
We can also identify Omicron on PCR tests. Usually a swab would have to go to a special lab for genome sequencing to know which variant caused the infection. However, it looks like Omicron has a special signal on the PCR directly. For example, when the PCR is positive it lights up two channels instead of three channels, indicating that it’s Omicron instead of Delta, for example. So why haven’t PCR tests caught Omicron in the U.S. either?
It may be that testing centers don’t know this handy trick yet
Maybe we have a positive PCR but it was sent to a lab for confirmation
Maybe we aren’t testing enough to detect a small number of cases
Or, there’s the possibility that it’s just not here yet
6. What about holiday plans?
During the onslaught of interviews today, many asked me about what Omicron means for the holidays. Can we still fly? What about holiday parties? Is Christmas cancelled? People… Let’s get through this next week. Once we have the data, we will know how to approach holidays smartly. But I have a hunch that it will include—can you guess?—masks, testing, ventilated spaces, and vaccines.
Love, YLE
“Your Local Epidemiologist (YLE)” is written by Dr. Katelyn Jetelina, MPH PhD— an epidemiologist, biostatistician, professor, researcher, wife, and mom of two little girls. During the day she has a research lab and teaches graduate-level courses, but at night she writes this newsletter. Her main goal is to “translate” the ever-evolving public health science so that people will be well-equipped to make evidence-based decisions, rather than decisions based in fear. This newsletter is free thanks to the generous support of fellow YLE community members. To support the effort, please subscribe here:
Thank you for the updates. It cuts through the noise and is timely and in depth.
Your updates are so helpful and clear. Thank you!