



Original antigenic sin: Are boosters a threat?

Many are trying to decide whether to get another booster. In order to make this decision, benefits must be weighed with risks. More than 11.3 billion doses of COVID19 vaccines have been distributed, so we are well aware that the vast majority of side effects are mild. Are there any other risks to getting another booster, like “original antigenic sin” (OAS)?
There has been considerable chatter among the public about OAS. From what I can tell, attention was sparked after an op-ed was published before Omicron. A few clinicians, including Paul Offit, said:
“It’s (...) possible that repeatedly “training” the immune system to fight the original virus could reduce the effectiveness of a variant-specific booster. This phenomenon, called “original antigenic sin,” has been observed with influenza and human papillomavirus vaccines. In other words, for those not in immediate need of a boost, there may be a significant advantage to waiting until a booster more closely aligned with circulating variants becomes available; boosting on the original antigen could be counterproductive.”
OAS is one of the most complicated and misunderstood parts of an already complex immune system. I partnered with Edward Nirenberg to “translate” the science:
What is OAS?
What is the science saying about OAS for SARS-CoV-2?
Is OAS a risk that should be weighed for a fourth booster?
Disclaimer: This post was incredibly difficult to write. My hardest since the pandemic began. It’s a very complex topic that even PhD immunologists get mixed up (and I’m an epidemiologist). This makes “translating” the topic even more difficult. I hope I don’t lose you. But if I do, just go to the “bottom line” section. Buckle up.
Original antigenic sin (OAS)
When we come in contact with a virus or get a vaccine for the first time, our immune system develops a repertoire of tools. One of those tools is B-cells, which are antibody factories. Each B-cell makes a single antibody shape, and they can pump out huge quantities of antibodies if needed. If you come in contact with another variant, B-cells can evolve and modify the antibodies they create for a new variant. This is just like factories that can modify their product on the line.
The immune system wants to clear a threat in the fastest way possible. Responses based on memory (as opposed to modifying the antibodies) work fastest, so B-cells get to work pumping out antibodies of shapes they’ve seen before. This is called “imprinting.” Imprinting in and of itself is neither good nor bad. It simply reflects that a person's first exposure to a virus can have a noticeable effect on their later responses to variants of that same virus.
Original antigenic sin (OAS) is a special type of imprinting. In OAS, prior memory can interfere and even prevent you from generating antibodies against new variants. How this occurs is not well understood.
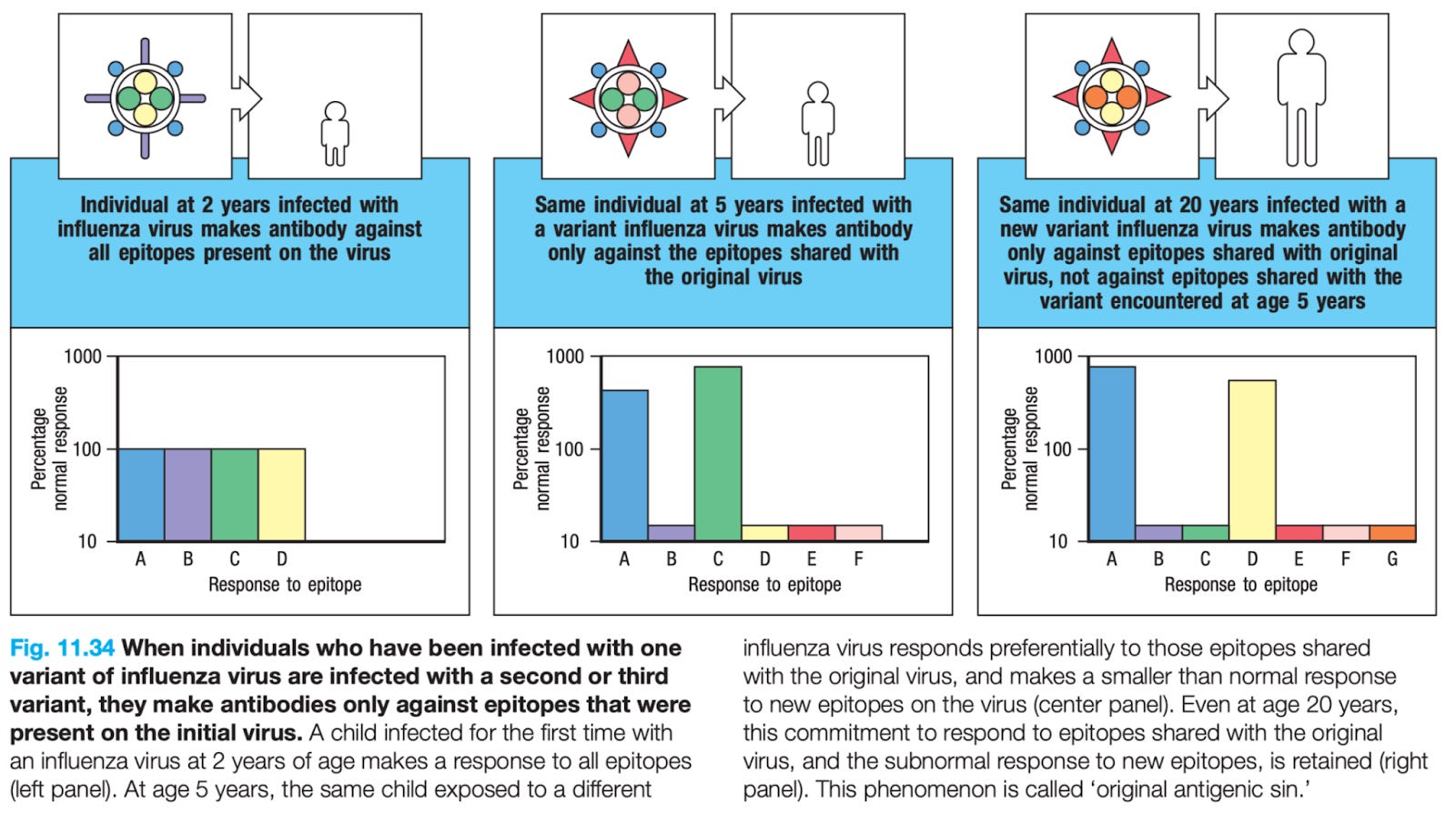
But we do know that OAS occurs with some other viruses, like the flu. For example, the first flu infection you get as a child has been shown to impact the way you react to flu variants later in life. While it could induce a less than optimal response, it can also be good and provide a more robust response. The figure below displays this phenomenon nicely.
Say a 2 year old is infected with the flu with A-D shapes on the virus. So, that child makes antibodies with A-D shapes. But then, at 5 years old, they are exposed to another variant with shapes A, C, E, and F. Because of the first exposure, only antibodies for shapes A and C respond. Even though there are only two shapes recognized, they provide a much stronger response than originally. Then, say at 20 years old, that same person is exposed to a virus with shapes A, D, E, and G. Because of the very first exposure (at 2 years old), antibodies A and D are recalled to fend off the infection; antibodies against E and G do not get made.
During the 1918 flu pandemic, we also saw very worrisome epidemiological signs of OAS. Those who were previously infected by the Russian flu (i.e. a different type of swine flu) did significantly worse during the pandemic than those not previously infected by the Russian flu.
Because we’ve seen OAS with other viruses, it’s theoretically possible with SARS-CoV-2. And scientific studies are now coming through.
What is the science saying?
The best way to analyze OAS is to look at someone who has never been exposed to SARS-CoV-2 (including through vaccination) and infect them with Omicron. Then, compare their immune response to someone who has been vaccinated and gets a breakthrough case. To my knowledge, this type of study has not been conducted. So we have to rely on proxy studies and assess OAS indirectly. So far, results are mixed.
On one hand, there is some evidence of OAS with SARS-CoV-2:
One scientific group found that exposure to coronaviruses (like the common cold) before the pandemic may impact our response to SARS-CoV-2. It’s important to note that there were significant internal inconsistencies with this study though. For example, the antibody levels weren’t correlating with severe disease when we would except they would.
Another group found that monkeys with a Beta-specific or Omicron-specific booster had no extra protection compared to a regular formula booster. This was surprising because Omicron has 32 changes on its spike protein compared to the original virus. So, one would hypothesize that a vaccine with an updated spike protein would provide some sort of additional protection. OAS may explain why it’s not working. Importantly, there could be alternative explanations of why this is happening, too. For example, there may have not been enough follow-up time or Omicron or Beta may simply not be as good at driving the immune response.
Then there’s science showing OAS only with infection and not vaccination:
One study found that SARS-CoV-2 infections caused B-cells to recall past coronavirus infection (like common cold) memory. But vaccines did not. So, infections recalled antibodies that couldn’t stop infections while vaccines recalled neutralizing antibodies. This could be because of location: COVID19 is inhaled—as opposed to vaccines, which are introduced in the muscle—causing less affinity.
On the other hand, there is evidence that OAS is not a concern for SARS-CoV-2 among humans.
An interesting study found OAS occurred in mice but not children. Specifically, scientists infected mice with the common cold and mice were unable to make antibodies against SARS-CoV-2. On the other hand, scientists found that children with a history of this common cold were able to make SARS-CoV-2 antibodies. In fact, they made higher levels of antibodies against SARS-CoV-2 if they had a history of the cold. This is the opposite of what would be expected from OAS.
Most recently a team from BioNTech evaluated 3 vaccine doses+infection compared to 2 doses+infection. They found that those with the 3 doses+infection had a higher number of neutralizing antibodies and created Omicron-specific B-cell memory. This suggests an “expanded imprint”—prior memory did not interfere with generating antibodies against new variants. Importantly, though, some level of imprinting was still present, as the majority of memory B cells were those from the original vaccine.
Data from a group of individuals in Stanford and Mongolia found that many COVID19 vaccines (not just mRNA) had extremely broad responses—significantly more so than those elicited by infection from specific variants, suggesting that the immune system has more paths of protection for new variants of concern.
A French group tracked the antibody response against SARS-CoV-2 over time in humans. They found that while initially B-cells recalled cold coronaviruses, they were successively replaced with SARS-CoV-2-specific antibodies. This, again, argues against a substantial role for OAS.
Can another booster make OAS worse?
It’s plausible that repeated boosting may make it harder to respond to future variants. Theoretically, repeated exposure to an older variant formula may drive our immune system to concentrate too much on old features and not on new features. But despite some truly surprising evolutionary leaps of the virus (like Omicron) we have not seen any convincing evidence of OAS among humans, which is great news.
In the event that OAS does prove to be a concern, there are tactics that vaccinology can take to work around it. For example, we are testing universal vaccines against SARS-CoV-2 and are fortunately seeing early promising results. Furthermore, flu scientists have found a way to boost immunity by targeting other areas of the virus. In a phase I study, scientists tested this strategy and OAS was not a problem for more than 1 year later.
Bottom line
After two years of vaccines and the virus significantly mutating, there is no definitive evidence of OAS in humans being an important concern for COVID-19.
Without knowing the future, decisions must continuously weigh benefits with risks we know right now. Evidence from Israel shows meaningful benefit of a fourth mRNA dose (or second booster) against severe disease among older adults. We need to be responsive to the needs of our immune systems to protect us from this virus. The reality is, for someone who needs a booster, the theoretical concern of OAS is not a strong enough reason to not get it.
Bottom bottom line
If you’re eligible, go get your booster.
Love, YLE and Edward Nirenberg
“Your Local Epidemiologist (YLE)” is written by Dr. Katelyn Jetelina, MPH PhD—an epidemiologist, biostatistician, professor, researcher, wife, and mom of two little girls. During the day she has a research lab and teaches graduate-level courses, but at night she writes this newsletter. Her main goal is to “translate” the ever-evolving public health science so that people will be well equipped to make evidence-based decisions. This newsletter is free thanks to the generous support of fellow YLE community members. To support the effort, please subscribe here:
Katelyn, You are doing an excellent job of informing everyone of factors to consider. I appreciate your effort.
This comment from a career MIcrobiologist(41 years)
I want to know if they're going to study this guy: https://www.kcrg.com/2022/04/03/man-germany-gets-90-covid-19-shots-sell-forged-passes/