

Pediatric numbers: 3 things to keep an eye on

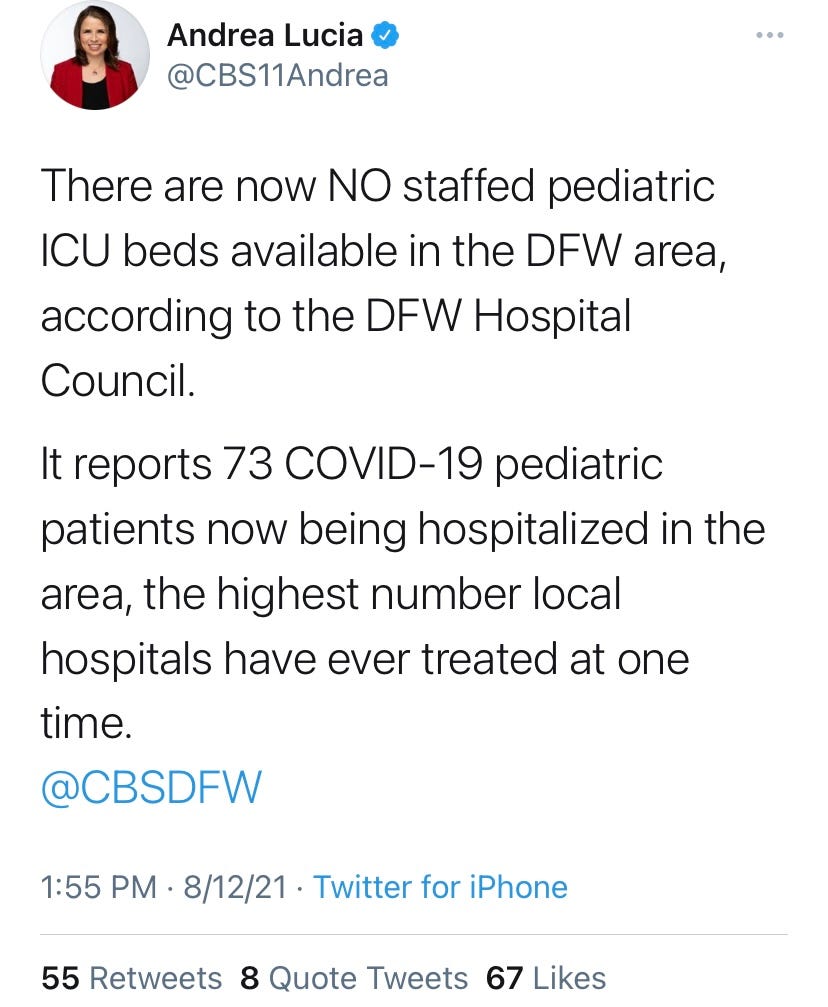
There’s no lack of anecdotal evidence that pediatric hospitals are reaching capacity in many states. This past weekend, Dallas had zero ICU beds for kids.
But, anecdotal evidence can be very different than population-level evidence. So, what are we seeing on a population-level? And, is there anything we should be concerned about?
Epidemiology
In the past…
