



Pediatric State of Affairs: April 28

There are several new developments that have come to the surface in the past few weeks for children. Here is an update for us parents out there.
Epidemiology
Omicron was a record-breaking wave, especially for children. At its peak, more than 1.15 million children were infected per week. The CDC reported that infection-induced immunity increased from 44 →75% among 0–11 year olds and 46→74% among 12–17 year olds from December 2021 to February 2022. This was a drastic increase, even compared to other age groups.

This wave did not come without suffering. More than 11,000 children were hospitalized in 25 states, and five times as many children ages 4 and younger were hospitalized compared to previous waves. Of the 5-11 year olds hospitalized during Omicron wave, 90% were unvaccinated, 30% did not have an underlying condition, and 20% required ICU admission. The disease profile also slightly shifted with Omicron. A JAMA study found Omicron was associated with a 3-fold increase in hospitalized Upper Airway Infections (like croup) compared to prior variants. During the Omicron wave, Kaiser Family Foundation reported COVID19 was the fourth leading cause of death for 5-24 year olds.
Importance of vaccination
High rates of infection will, no doubt, help build an individual- and population-level immunity wall. This is especially true if your child was vaccinated. We’ve had 30+ studies showing that “hybrid immunity” is superior compared to either vaccine or infection alone. This is not a reason to go purposefully get your child infected, but it is a strong viable path to protection.
Unfortunately, only 35% of 5-11 year olds and 68% of 12-17 year olds have one dose of the vaccine. That also means a whole lot of parents are relying on infection-induced immunity for their children’s protection. There are three big reasons why I wouldn’t rely on this protection in the face of Omicron:
Neutralizing antibodies, our first line of defense, don’t stick around for long. Before Omicron, the rule of thumb was 90 days but this has probably shortened due to Omicron continuing to mutate to escape immunity. The most recent sister lineage, BA.2.12.1, is rapidly gaining speed in the U.S. and its two new mutations further escape immunity. BA.4/BA.5 (which are circulating in South Africa) have the same mutation, too. We are confident that Omicron will continue to mutate to chip away at immunity.
Perhaps more importantly, we’re seeing Omicron-induced immunity among unvaccinated people does not protect against other variants of concern, like Delta (here, here, here). In the New England Journal of Medicine article, those with an Omicron infection had incredibly low cross-reactivity (i.e., in the Figure, the circles are lower in Panel B compared to the other panels). In other words, an Omicron infection didn’t provide broad protection against future infections from other known variants. While Omicron may be the only variant circulating right now, that certainly can change in the future. And if, for example, another Delta variant came along that is far more severe, these kids may be out of luck.
Your child’s Omicron infection may have induced B-cell and T-cell defenses too, which help protect against future severe disease and death. However, this is not guaranteed, especially with Omicron. The quality of response (i.e. memory B-cells and T-cells) is relative to the severity of infection. If a child had a mild infection (which many do), then they likely had a lower viral dose, and that secondary protection is less likely.
We want our kids to have the broadest, strongest immunity wall they can have. And this can be achieved through vaccination.
Under 5’s Vaccine
This evidence also highlights the importance of getting kids under 5 vaccinated. The most recent vaccine timeline has been largely comprised of whispers on the street, but this is what I’ve gathered:
Moderna: On March 24, Moderna announced that their pediatric vaccines worked. The efficacy wasn’t ideal (48%), but expected with Omicron’s ability to escape immunity. Today they officially applied for an EUA after a few weeks of addressing incomplete paperwork. It typically takes the FDA 5-6 weeks to review everything (It took them 5 weeks to review Pfizer’s 5-11 vaccine), but maybe they will take this opportunity to step on the gas! If they don’t, this would land us in mid-June for the VRBPAC meeting.
Pfizer: Concurrently, we’re waiting for third-dose Pfizer data. I would assume Pfizer is working in overdrive to get their data analyzed and submitted. I’m a little surprised we haven’t heard anything yet, which is making me a little nervous about the effectiveness of their third dose. Nonetheless, if and when Pfizer turns their data over, the FDA will review it. Because the FDA already has their two-dose data, I would assume this would be faster than Moderna.
So, it’s possible that both vaccines would be reviewed at the same VRBPAC meeting in June. If Pfizer doesn’t submit their data in time, it’s 100% reasonable (and should be 100% expected) that the FDA would go forward without Pfizer. I’m optimistic we will have a vaccine by June.
Treatment
While we anxiously wait for a vaccine, we finally got the first COVID19 treatment for children under 12. On Monday, the FDA expanded the approval of Remdesivir (official name is Veklury) for children 28 days and older and weighing at least 7 pounds. This drug slows down viral replication in our cells, which allows the immune system to fight the virus more effectively and quickly. A clinical study of 53 hospitalized children received Veklury for up to 10 days, and it was shown to be safe and effective. Remdesivir is approved only for children hospitalized with COVID19.
Bottom Line
With an Omicron sweep, it’s still incredibly important to get kids vaccinated. Thankfully, this is coming for us parents with kids under 5. In the meantime, we have other tools that work, like treatments, boosters, antigen tests, and masks. For some reason, a vaccine seems like the finish line of this exhausting two-year road as a parent. And I couldn’t be more excited that it’s finally on the horizon.
Love, YLE
“Your Local Epidemiologist (YLE)” is written by Dr. Katelyn Jetelina, MPH PhD—an epidemiologist, biostatistician, professor, researcher, wife, and mom of two little girls. During the day she has a research lab and teaches graduate-level courses, but at night she writes this newsletter. Her main goal is to “translate” the ever-evolving public health science so that people will be well equipped to make evidence-based decisions. This newsletter is free thanks to the generous support of fellow YLE community members. To support the effort, please subscribe here:
"The CDC reported that infection-induced immunity increased from 44 →75% among 0–11 year olds and 46→74% among 12–17 year olds from December 2021 to February 2022."
Given the general understanding of what "immunity" means, I think that characterization of what the CDC reported is misleading. What they reported was an increase in the seroprevalence of infection-induced SARS-CoV-2 antibodies, not immunity. While there is a strong correlation between the presence of SARS-CoV-2 antibodies (infection-induced or vaccine-induced) and immunity against a SARS-CoV-2 infection (or reinfection), one could have such antibodies (especially at low titers) and not be immune to a SARS-CoV-2 infection.
Some questions and feedback:
1) KJ: "More than 11,000 children were hospitalized in 25 states, and five times as many children ages 4 and younger were hospitalized compared to previous waves."
How do these rates compare with general hospitalization rates for children for other ILI respiratory viruses during flu season? 11,000 sounds like a large number, but it probably only represents between 2%-6% of pediatric hospitalizations, no? Sources I've found indicate roughly 150,000 non-neonatal pediatric hospitalizations per month can be expected, though it doesn't break down by cause only noting "Respiratory diagnoses—pneumonia, acute bronchitis, and asthma; mood disorders; appendicitis; and epilepsy/ convulsions were the most common specific conditions for which children were hospitalized" [1]. CDC indicates in the < 5 cohort alone as many as 26,000 hospitalizations in a flu season [2]. How much higher was hospitalization rates during Omicron than baseline? Than high flu seasons like 2017?
2) KJ: "Of the 5-11 year olds hospitalized during Omicron wave, 90% were unvaccinated, 30% did not have an underlying condition, and 20% required ICU admission."
Is this statistically significant considering when the study began 80% of the 5-11 cohort was unvaccinated and by the time the period ended 7 out 10 were still unvaccinated? [3] Isn't this a base rate fallacy? Especially once you break by ethnicity and the rates converge?
Additionally, the study period is 14 weeks yet they group partially vaccinated along with unvaccinated which as they admit as one of the limitations: "Third, analyses based on vaccination status are biased toward the null because partially vaccinated children were grouped with unvaccinated children." < there was no reason to do this, they had the data to break cohorts. And a previous version stated they also included anyone who was fully vaccinated but got covid within 2 weeks of 2nd dose as "Unvaccinated" as well, though a stealth update removed that verbiage. That makes this far less impressive.
No to mention "There were no significant differences for severe outcomes by vaccination status." undercuts the benefit of a non-sterilizing vaccine.
3) KJ: "The disease profile also slightly shifted with Omicron. A JAMA study found Omicron was associated with a 3-fold increase in hospitalized Upper Airway Infections (like croup) compared to prior variants."
Is there possibility the increase was due to children returning to school in far greater numbers after a large % of the country missed school in 2020-2021? (Pre-Omicron period studied was March 1, 2020, to December 25, 2021 compared to December 26, 2021, to February 17, 2022 for Omicron) Scanning other countries which didn't participate in the "keep kids out of school" approach (half of Europe, all Nordic countries, etc) I am not finding papers noting rising UAI in these countries (easily could be I am simply missing the research, so if anyone finds something please link).
Also, the "3 fold increase" is relative increase, overall the absolute increase of +2.6% seems unremarkable considering the sampling methods.
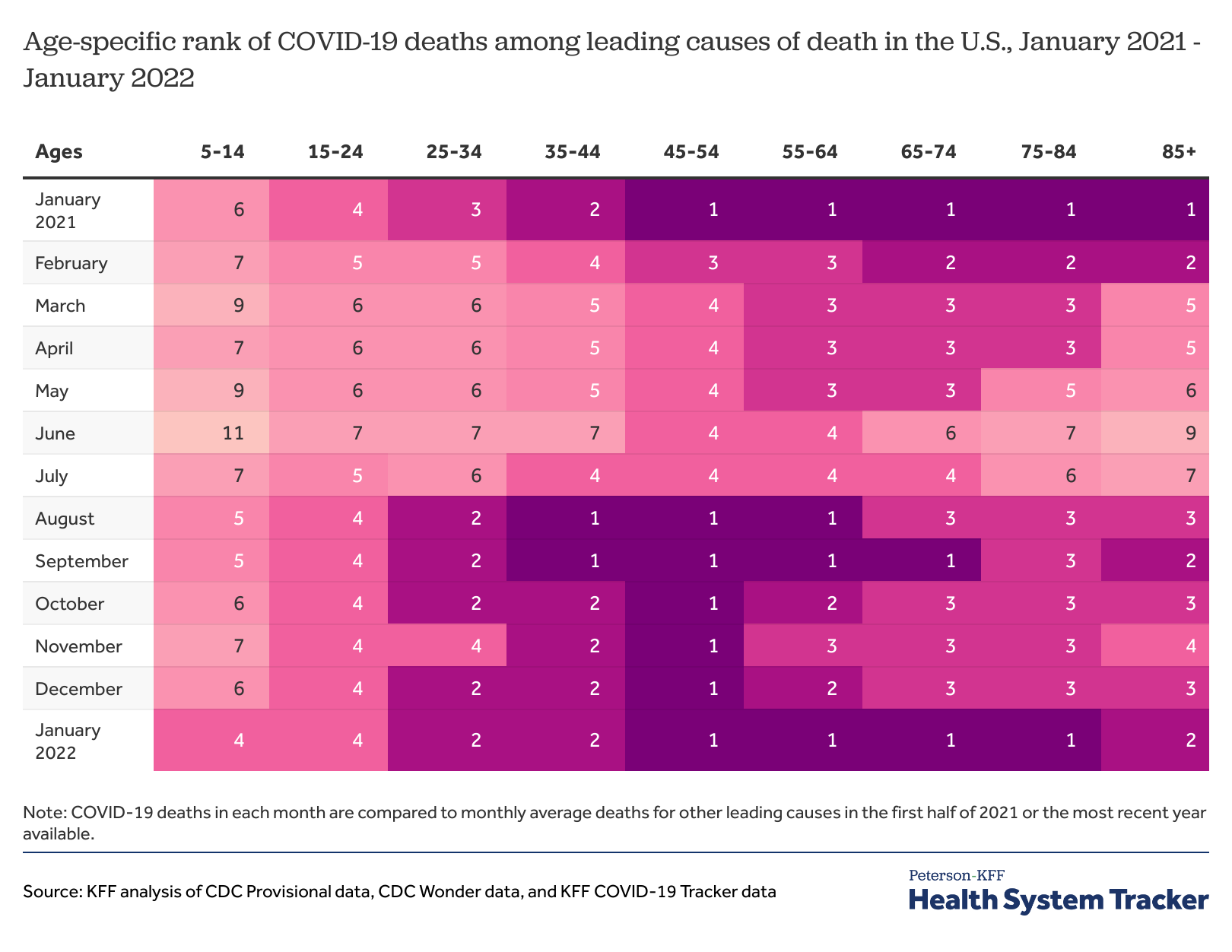
4) KJ: "During the Omicron wave, Kaiser Family Foundation reported COVID19 was the fourth leading cause of death for 5-24 year olds."
That would be notable if there were say, 100 different causes of deaths in that age cohort normally distributed. Then ranking #4 would be noteworthy. Instead, there are between 10-15 causes deaths (depends how you group accidents mainly how granular you want) with a front loaded pareto distribution. A more accurate phrasing would be "During the Omicron wave, COVID19 accounted for 1.3% of deaths for 5-24 year olds". The rise in homicides, overdoses, and suicides in this age group I believe is the larger concern, as it accounts for nearly all excess deaths in that cohort.
5) Regarding the infographic from the Health System Tracker, how do we reconcile the fact that Covid bounced back to the #1 cause of death for 65+ despite being 95% vaccinated? Credit was given to the vaccine as Covid dropped from #1 to #6 between Jan 21 and June 21, but now that it climbed back to #1 what is the explanation?
6) KJ: "With an Omicron sweep, it’s still incredibly important to get kids vaccinated. Thankfully, this is coming for us parents with kids under 5."
In Sweden, they don't recommend the vaccine for children under 18 without comorbidities. Despite this and other controversial approaches (kids back in school May 2020, kids not masking, overall the lowest masking rates in the world for adults, limited lockdowns, etc) they have among the best outcomes in the world with zero excess deaths under age 75 throughout the entire pandemic [4] and the 2nd lowest total excess deaths worldwide (only beaten by Norway).
How to reconcile that outcome with our approach which placed us as the leader in excess deaths?
7) Why did the CDC MMWR not report on prior infection status? That is, how many of the hospitalized children were there with a repeat infection? They certainly had this data given the charts they accessed, why not detail it?
8) Why did the CDC fail to break down comorbidities by vaccination status? Again, they had this info but neglected to present it. I can only assume they left it off because it made no difference.
9) Considering 5-11 vaccination was only approved November of 2021 and this study is Dec-Feb, doesn't the data from this report actually show the vaccine only has a 50% efficacy and wanes quickly given how many vaccinated children were still hospitalized?
Appreciate any feedback, thanks!
[1] https://www.hcup-us.ahrq.gov/reports/statbriefs/sb187-Hospital-Stays-Children-2012.jsp
[2] https://www.cdc.gov/flu/highrisk/children.htm
[3] https://data.cdc.gov/Vaccinations/COVID-19-Vaccination-and-Case-Trends-by-Age-Group-/gxj9-t96f
[4] https://imgur.com/a/Pbuu0rI - you can recreate using Tabell 2 from https://www.scb.se/en/finding-statistics/statistics-by-subject-area/population/population-composition/population-statistics/pong/tables-and-graphs/preliminary-statistics-on-deaths/