



Up, up, and away
Respiratory State of Affairs: December 19

Welp, I’ve spent the past two days on a couch with my 4-year-old, who has the flu. Who knew a toddler could watch 10,000 Disney princess movies and still have an appetite for more? Respiratory season is here. Apparently so is our princess era.
There are many viruses circulating right now, but we aren’t at peak season yet. Here’s the State of Affairs so you feel well-equipped for the holidays.
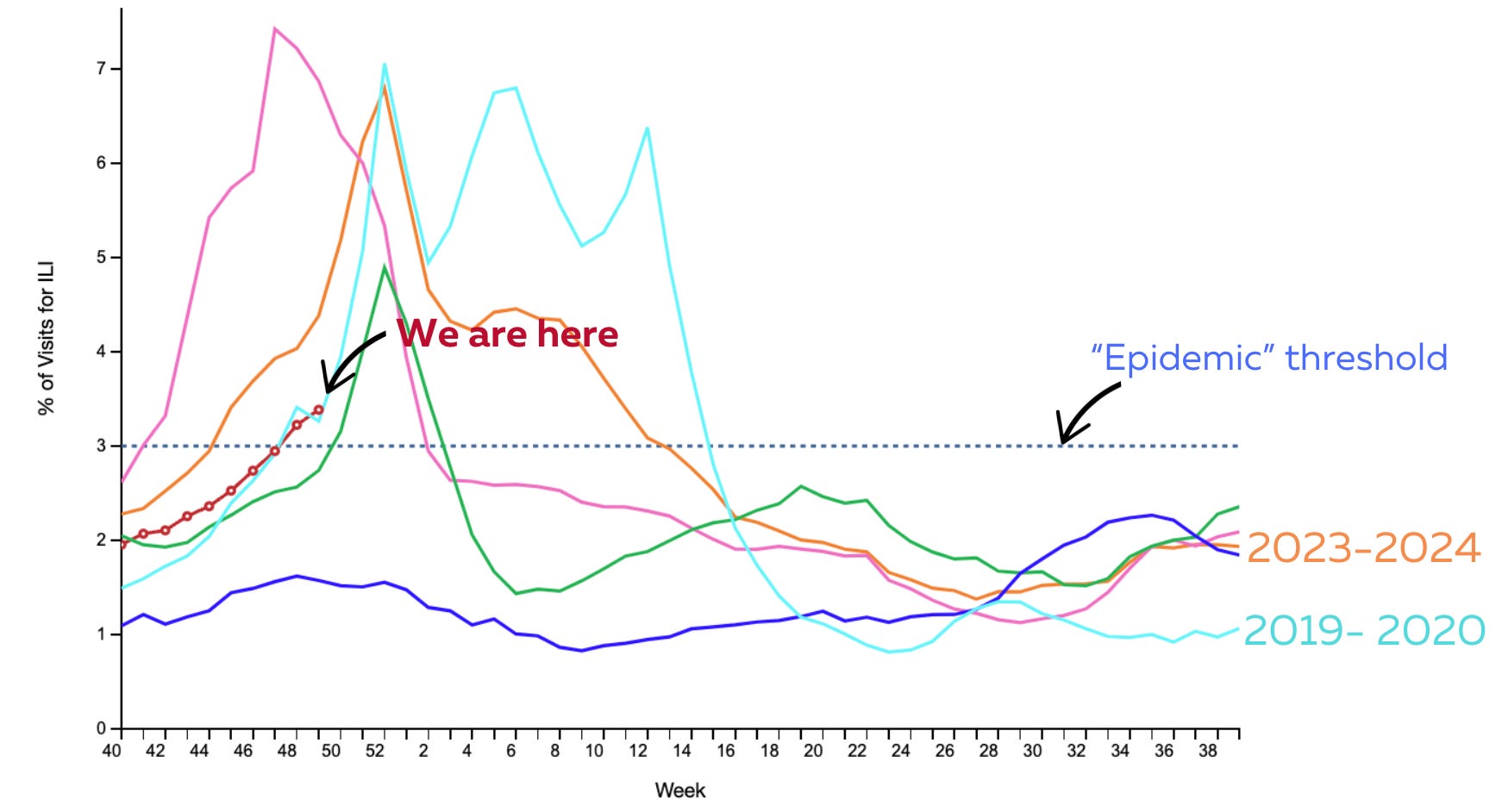
Influenza-like illnesses: Moderate and increasing
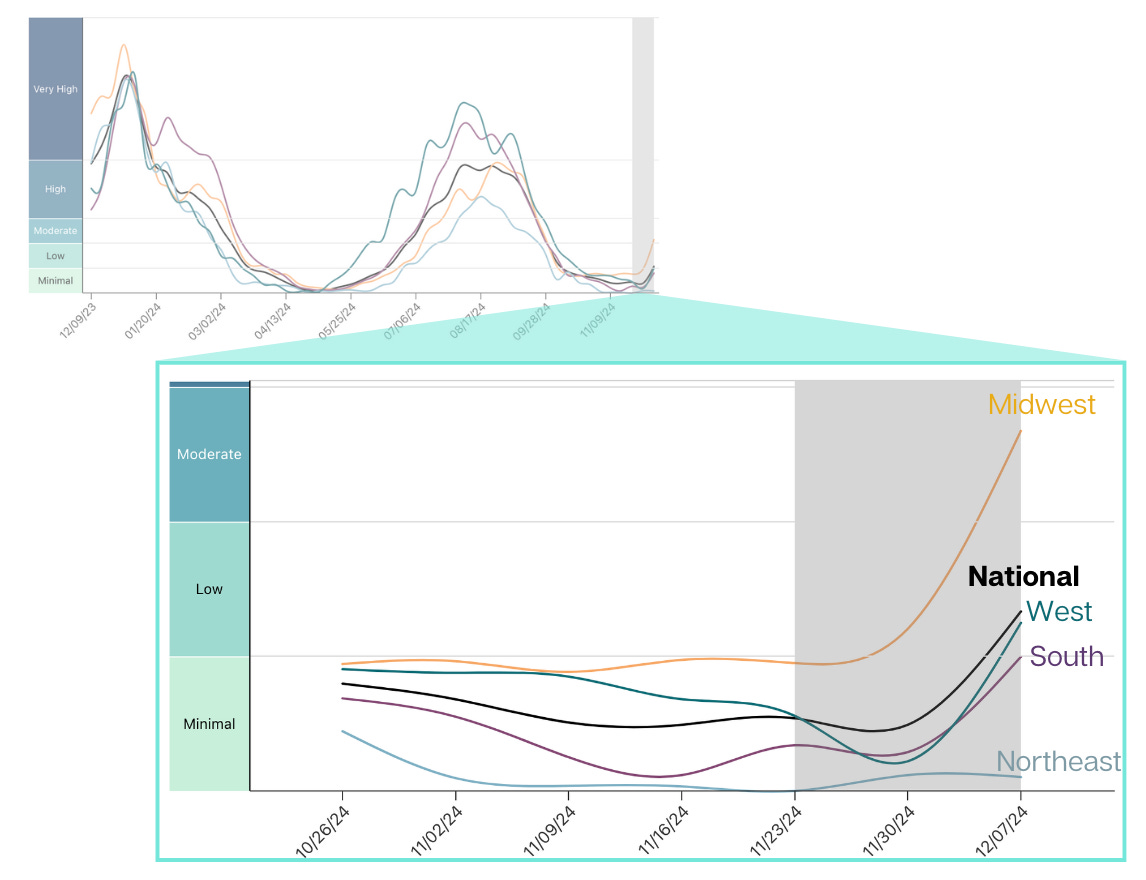
The climate of respiratory health in the United States—which the CDC defines as “influenza-like illnesses” (ILI)—has crossed the “epidemic” threshold and is growing. The trend seems to be tracking exactly with the 2019-2020 respiratory season. I’ve started wearing my mask while traveling.
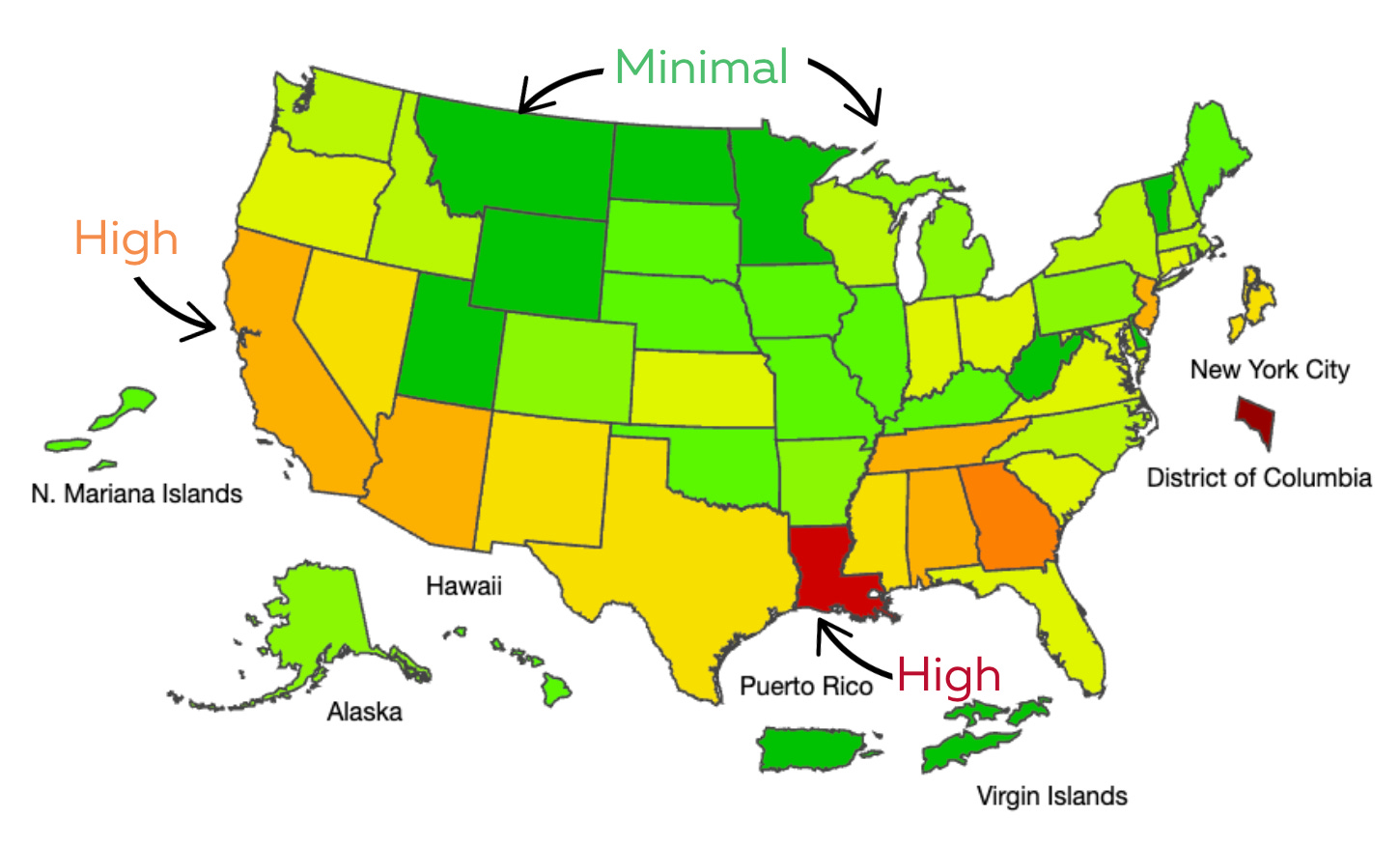
ILI has lit up in the West and South. The Midwest is still pretty quiet. Eventually this entire map will be red and purple.
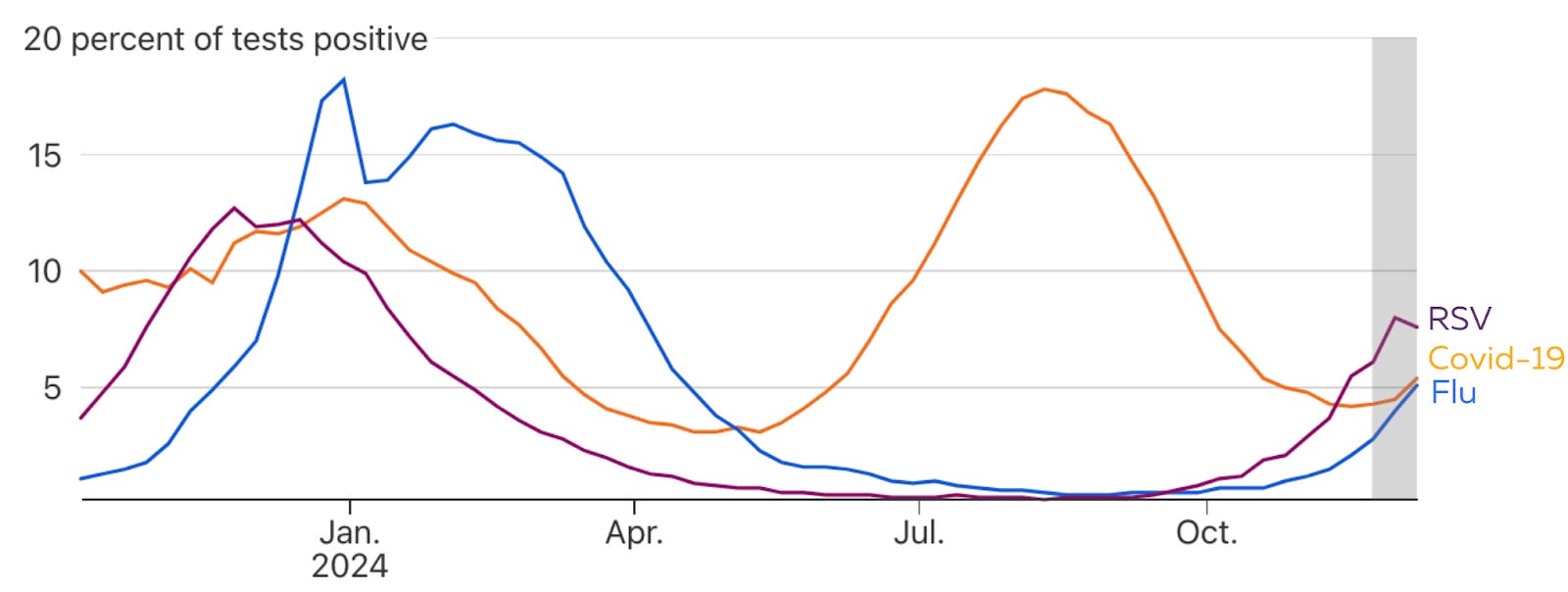
Flu: Moderate and increasing
Flu is coming in hot, with an exponential spread across the United States. The spread is mainly due to Flu A strain; we typically see a Flu B peak in early spring. Nothing abnormal is jumping out about this year yet.
However, one concerning trend is flu vaccine coverage—it’s getting lower and lower every year in a step-wise fashion. This may explain last year’s high flu deaths among kids.
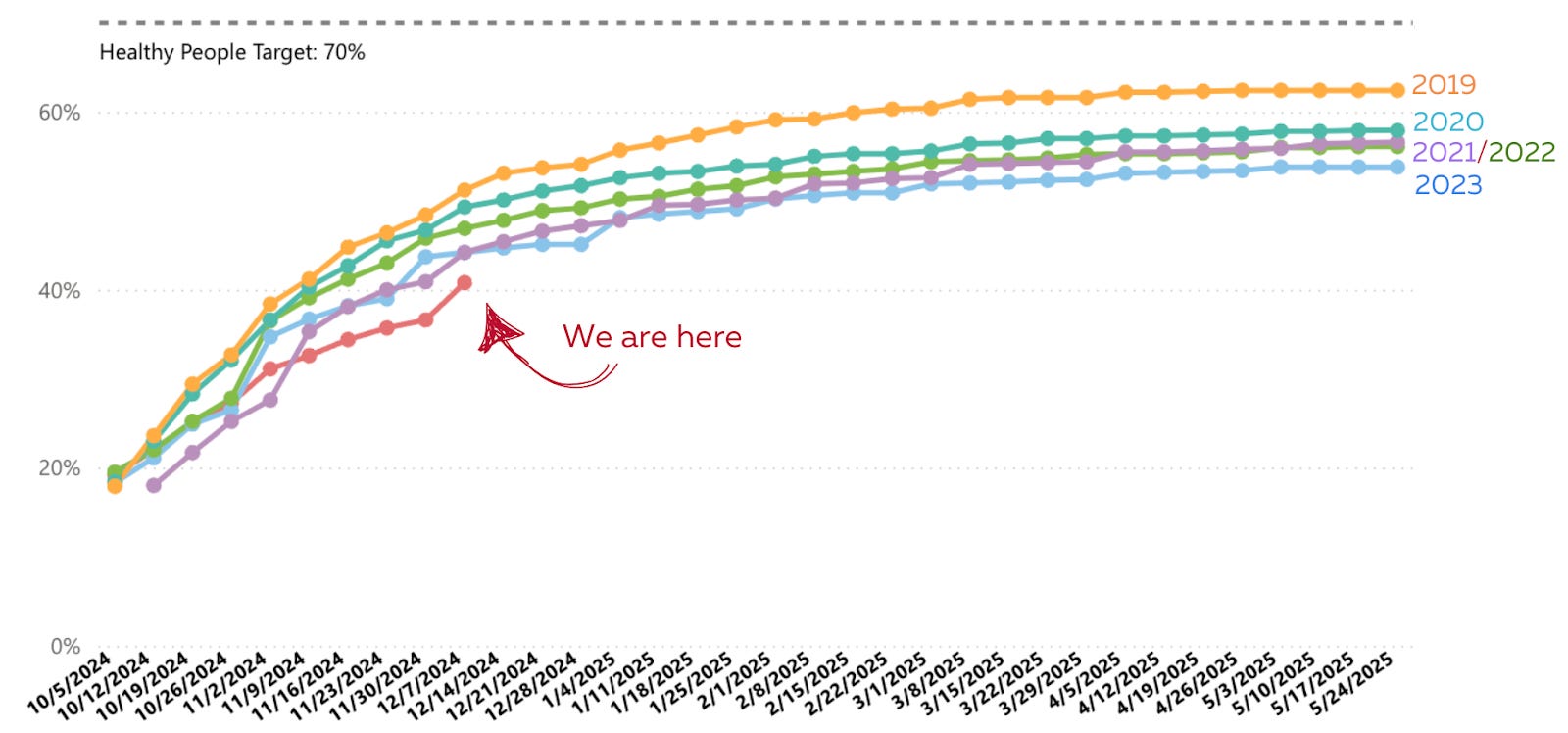
My daughter was vaccinated against the flu but still got infected. Unfortunately, the flu vaccine may not be a great match this year (~34% effectiveness in the Southern Hemisphere) because a specific strain is circulating. Regardless, a flu vaccine helps bring sickness from wild to mild. It’s not too late for a flu vaccine.
Also, hot tip: We used an at-home combo flu/Covid test. I wouldn’t normally care which virus infected her, but with flu, there is a specific action to take—a prescription for Tamiflu can help relieve symptoms one day earlier. This saved us a trip to the pediatrician’s office!
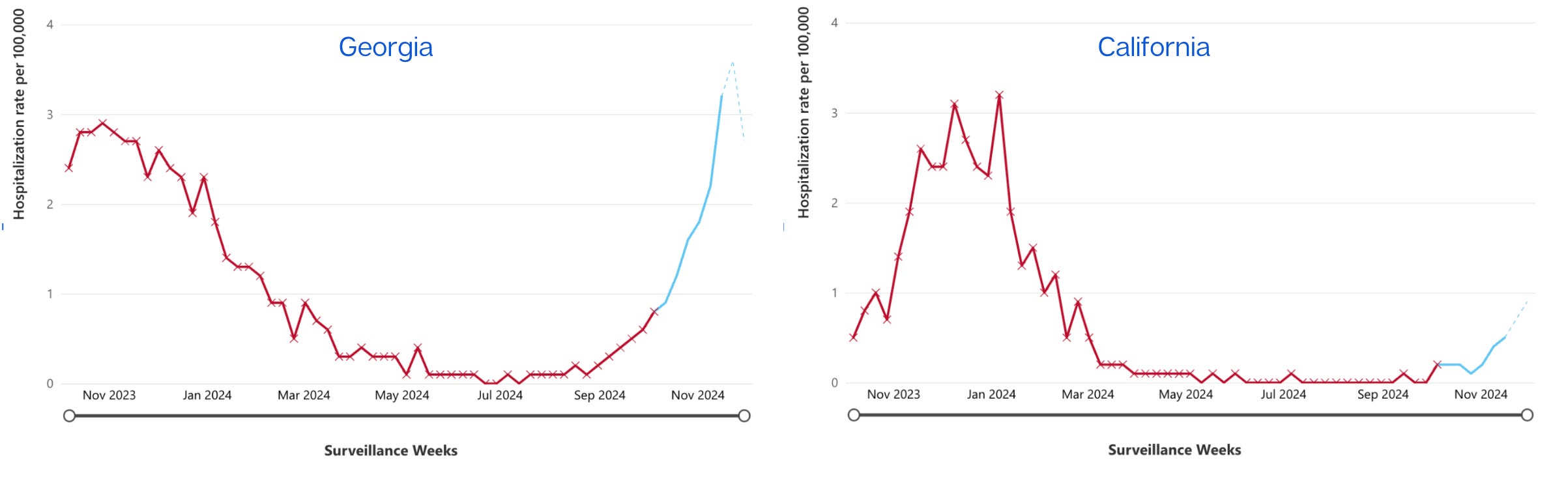
RSV: Peaked in some areas?
RSV may have peaked in the East/Southeast, like in Georgia, but definitely still increasing in other states, like California. This is typical of RSV—waves start in the Southeast corner and spread outward nationwide. Scientists don’t really know why.
So far, we are having a middle-of-the-road season for RSV. I’m curious if/when we will see a population-level impact from RSV vaccinations and monoclonal antibodies. It doesn’t seem like this year is the year.
Covid-19: Low but increasing
Some epidemiologists were quietly questioning whether it was possible to have a no-Covid winter, given low activity over the past month or two. Historically, Covid-19 has started increasing in November and peaked around the first week of January.
However, those rumblings were put to rest this week as Covid-19 wastewater started increasing again. Levels are still relatively low but growing.
My guess is that this winter’s Covid-19 wave has just shifted—it will peak in February. Given the relatively large summer wave, we’ll have a smaller peak than previous winters. We’ll watch to see if Covid-19 has any surprises for us.
Increasing Covid-19 (and other viruses during the winter) is largely due to three factors:
New variants. The latest Covid-19 variant is called XEC, and it has a few mutations that allow it to skip around our first line of defense, causing infections. Its growth advantage isn’t too big at 20-45%. (As a comparison, Omicron was 500%.) This signals the winter will be a wave, not a tsunami.
Cold weather leads people inside, which has poor ventilation. Also, some weather properties, like humidity, increase transmission.
Social networks. With the holidays, we see people we wouldn’t normally see, allowing viruses, like Covid-19, to transmit more.
If you’re one of those trying to time a Covid-19 vaccine before a wave to optimize protection against infection, the time to get vaccinated is now.
Other things going around
Walking pneumonia is still high but finally decreasing after a nasty year. This causes a lingering cough that is typically not severe but a nuisance.
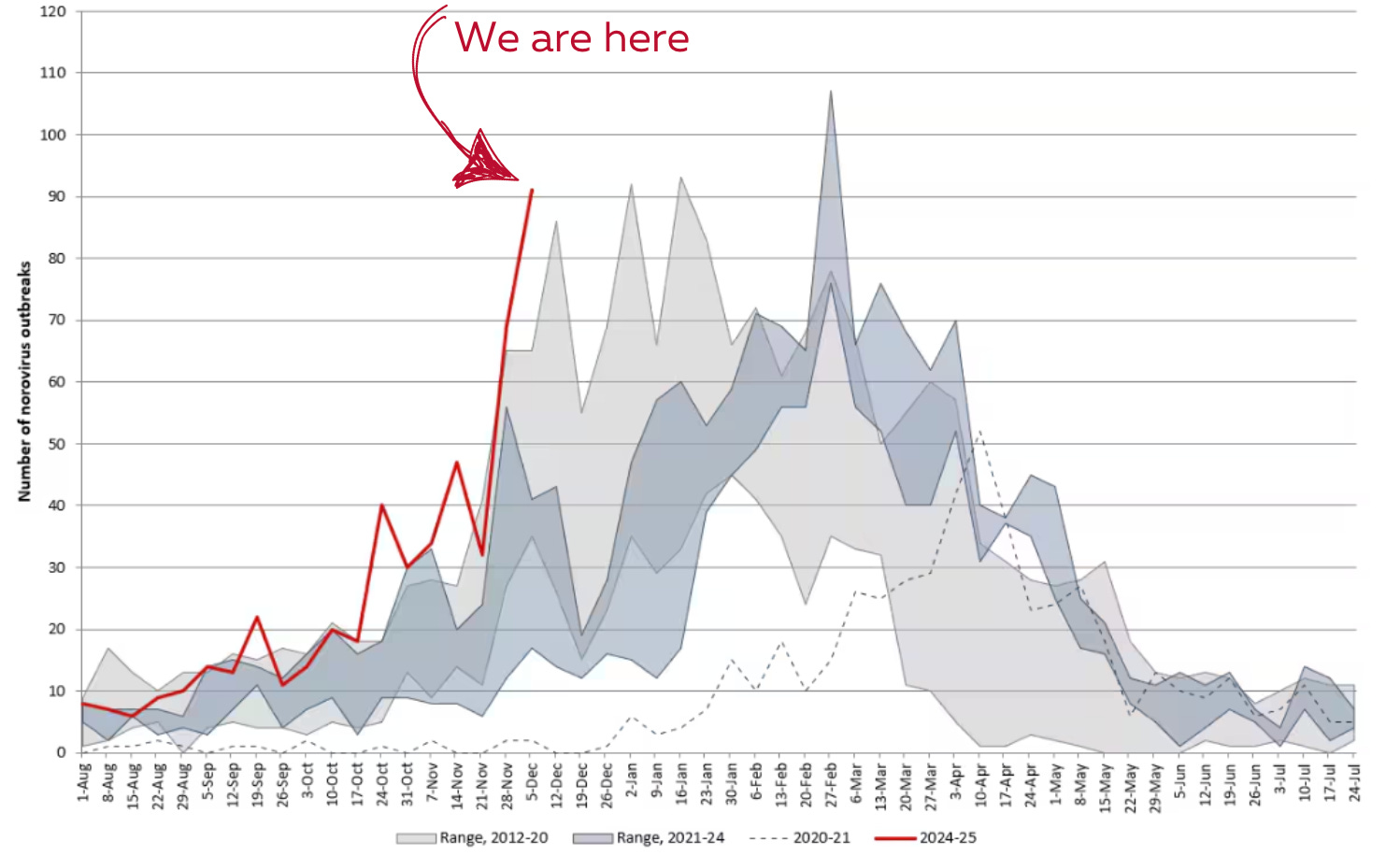
Norovirus—think nausea, vomiting, diarrhea—is having quite the time, with the number of positive tests and outbreaks abnormally high. Norovirus spreads through contaminated surfaces, so as always, wash those hands. Unfortunately, this virus is one of the hardest viruses to kill because it doesn’t have a stable coating called a membrane. So, a quick dose of hand sanitizer doesn’t work. Bleach-based products on surfaces are the best. Read more in a previous YLE post.
Whooping cough is back to pre-pandemic levels, though it’s preventable with the Tdap/DTaP vaccine. According to a recent survey, a third of the public doesn’t know this disease is preventable. Adults need boosters—one every 10 years. Unfortunately, our second-generation vaccines are imperfect, and vaccine hesitancy is rising.
H5N1 (bird flu)— Despite all the headlines this week, nothing much has changed for the general public: The virus keep spreading, severe cases are starting to pop up (latest in Louisiana) from people with direct contact with sick animals, and, thankfully, more resources are being channeled to public health (see CA State of Emergency). It’s clear this virus isn’t going away any time soon. The biggest concern is the potential for a mutation, especially since seasonal flu is now circulating. H5N1 could swap genes with seasonal flu and become more susceptible to humans.
Bottom line
Things are heating up! Stay healthy out there— get vaccinated, get that air moving, use masks, and stay home if you’re sick. (And if you’re stuck at home watching Disney movies like me, I highly recommend starting with Encanto).
Love, YLE
In case you missed it:
Your Local Epidemiologist (YLE) is founded and operated by Dr. Katelyn Jetelina, MPH PhD—an epidemiologist, wife, and mom of two little girls. During the day, Dr. Jetelina runs this newsletter and consults with several nonprofit and federal agencies, including CDC. YLE reaches more than 290,000 people in over 132 countries with one goal: “translate” the ever-evolving public health science so that people feel well-equipped to make evidence-based decisions. This newsletter is free to everyone, thanks to the generous support of fellow YLE community members. To support the effort, subscribe or upgrade below:
I read and subscribe to your newsletter. I have followed you since the heart of the SarsCov2 pandemic and am beyond grateful for your hard work and advocacy. Thank you for what you do.
I have a question I'm hoping you'd be willing to chew on, coming from a place of respect, appreciation, and genuine pleading for myself and my community:
Why don't you mask year-round in public spaces? Like grocery stores, doctors' offices, drugstores, transportation, etc?
A large chunk of people are naturally immune compromised. Or on immune suppression. Or have autoimmune conditions. Etc. As an epidemiologist, you are intimately aware of how one-way masking of the vulnerable individual can only go so far. Especially in an abysmal air filtration, testing, and infectious disease conscious landscape like the one we exist in currently.
My community and I have just as much of a right to exist in public spaces as those with more health privilege. The actions of nearly everyone unmasked just tells us that our furthering disability and death is not important enough. The general public, even our own friends and family, would rather us absorb that harm than take accountability for their personal role in the transmission environment they create. People would rather let us die than put a mask on.
We are put not only at physical harm, but at emotional harm. These actions tell us that we are second-class. Expendables. And I'm sure I don't need to tell you that the cumulative impacts of this over our lifetimes just sets us up for more suffering.
Why not become part of the solution and safety net for us? It is one of the easiest and most effective ways of helping lower infectious disease transmission of all kinds.
Your public clout is vital to our visibility and protection. If someone like you takes up this cause, it gains more legitimacy and traction. A cause, however legitimate, can only championed so far by the people it most impacts. Those of privilege and the larger community must pick it up if we are to matter. You are our bridge.
Would you be willing to set the trend and be an ally to a forgotten community?
Thank you for these important updates! Ob/Gyn here. FYI any adult around a neonate should have an updated Tdap to protect newborn from exposure.
(I remember when my tetanus is due based on granddaughters’s birthdate)
we also stress importance of RSV vax to pregnant women in 3rd trimester as immunity crosses placenta and has some protection for newborn as there’s no vax for them.