
Variant update

Well, my power came back on! At least for now.
And I was flooded with variant news. In an effort to keep organized, I scribbled down my thoughts. Here they are.
Bad news first.
In regards to B.1.1.7 (first detected in the UK)…
1,277 cases detected across 42 states. We know this is a gross underestimation, though, because of our suboptimal surveillance system in the US
People infected with B.1.1.7 have considerably higher viral loads, which could explain the higher transmissibility
B.1.1.7 has mutated once more. In fact, it has a new mutation called E484K, which is the exact trouble mutation that the South Africa variant and Brazil variant contain. This is terrible news because B.1.1.7 was the “tame” variant until now
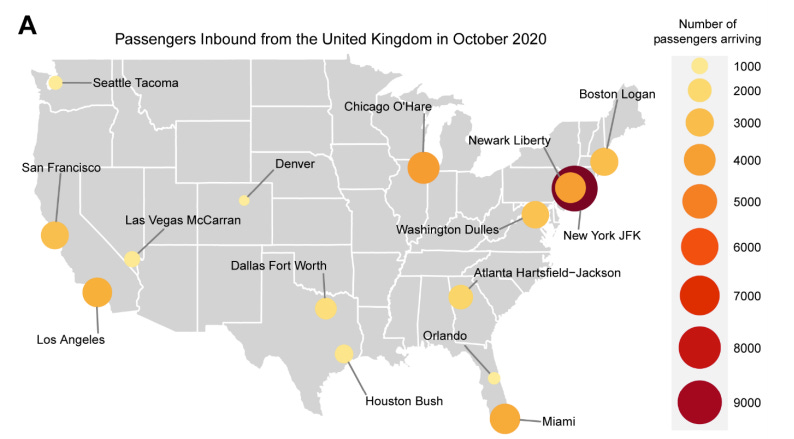
A few scientists looked at data from inbound flights in order to help predict where we are undercounting B.1.1.7. There were 3 take home messages:
73 people introduced B.1.1.7 into the U.S. This is high considering deceased travel and testing requirements from the U.K.
NY acted as a B.1.1.7 hub, as this is where 12 people from the U.K. introduced the variants separately. This isn’t a surprise, though, because NY is the main hub for U.K. travel overall.
TX, IL, and NJ had relatively high levels of U.K. travel but reported low cases of B.1.1.7. This variant is likely under-detected in these three states.

In regards to B.1.351 (first detected in South Africa)…
19 cases detected across 10 states
A test tube study found that B.1.351 reduces the number of neutralizing antibodies made from both “naturally” infected people and “vaccinated” people. This is the second study to find this, so it’s not surprising. But consistency is important. We still don’t know the impact on efficacy; we need a “real life” study to measure this. Reduction in neutralizing antibodies means an efficacy reduction by “a little” but not by “a lot”. Our vaccines will still work.
We’re slowly learning about B.1.351 transmission rates. A new study described the situation in Zambia. After 3 months of low counts, cases started increasing at an astronomical rate in mid-December. It just so happens that this is also when the country first detected B.1.351 (December 16-23, 2020). In the beginning of December, there were 44 daily cases. Exactly one month later (January 1-10, 2021) there were 700 daily cases (a 16-fold increase). This is very bad news as the variant starts to gain speed across the globe
In another test tube study, scientists found that B1.351 can completely escape monoclonal antibody treatment (bamlanivimab). In other words, this type of COVID19 treatment will not work if someone is infected by this variant. Another study found this too. We need to start updating the treatment cocktails so they can continue to effectively fight the virus.
Andddd there’s a new variant to pay attention to…
Called CAL.20C. First detected in southern California in October 2020. It, too, has mutations on the spike protein. So we need to pay attention to it.
A study found a correlation between the fast rise of CA cases and an increase in this new variant
It has now spread to 26 states and other countries (including Australia and U.K.)
Now, the good news.
B.1.1.7 does NOT seem to be more deadly or severe for children. This study directly contradicts the early mass media reports.
T-cells are going to help us out a lot with the new variants.
A new study found that even though vaccine efficacy isn’t as high with B.1.351 or P.1 and monoclonal antibody treatments don’t work as well (or at all), severe disease is still reduced at an equivalent level as old variants. It seems that this is due to our T-cells holding up. Unfortunately, variants can continue to mutate, and thus may not always be the case, but we take this as a big win.
Another study found that T-cells last up to 8 months (because the study was 8 months long). The authors concluded: “Development of medium or long-term protective immunity through vaccination might thus be possible.”
Our vaccines still work against all variants detected thus far (worth repeating)
Bottom line: Mutations are spreading. Our vaccines still work, but this may not always be the case in the future. Treatments are NOT working against these new variants, so we need to adjust these.
That’s “it” for now. Hopefully my power stays on for another update soon.
Love, YLE
Thank you for the time, dedication and energy you have put into keeping us informed. I am wondering if there is any information on covid’s affect on a person’s lungs in the cases occurring in people that have been vaccinated. I have seen articles about unvaccinated mild cases having lung Xrays that look like smokers lungs. I wonder if the same long term damage occurs in the cases of covid in vaccinated patients.
I am curious. In the US, how are they tracking the new variants? Is it mainly based on hospitalized patients who are not responding to monoclonal antibodies treatment and Covid reoccurrence on patients who were previously infected? Thank you for your time.