


A response to Florida Surgeon General's anti-human remarks
A response to Florida Surgeon General's anti-human remarks


This week the Florida Surgeon General said he is “very uncomfortable recommending the new Covid-19 vaccine to anyone” as it’s “anti-human.” Many of you have sent me this Fox News article that outlines his justifications.

He doesn’t have the greatest track record of making evidence-based vaccine recommendations. But as always, each claim should be evaluated individually based on its merit.
Let’s dig in.
Criticism #1: There’s no clinical data for the updated vaccines.
This fall, we do not have randomized controlled trial data for the updated Covid-19 vaccine. We didn’t have it last fall either. That is true.
But three critical points are missing from his argument:
We do have clinical (human) data. Moderna evaluated the human response to the updated vaccine in a lab, and the updated vaccines were found to significantly increase antibodies.
The changes from the last vaccine are small, literally the difference of a few amino acids—like a few letter edits on a Word document. We aren’t changing the number of words in the paper (like dosage of RNA), or the platform (like Word to Excel). Because of this, we are confident safety data largely reflects the billions of other mRNA doses already administered.
While randomized-controlled trials are the gold-standard evidence, it is not feasible to run them for everything (especially for a mutating virus). Conducting a Phase III effectiveness trial takes time, effort, and resources. The virus has already mutated by the time it’s over, and then we need a new formula. So we have adapted Covid-19 to our flu model. There is also an ethical concern with randomized trials—if we know the vaccine helps, is it ethical to give a placebo randomly to people?
Criticism #2: Side effects
Yes, some risks are real. But others are not.
Myocarditis
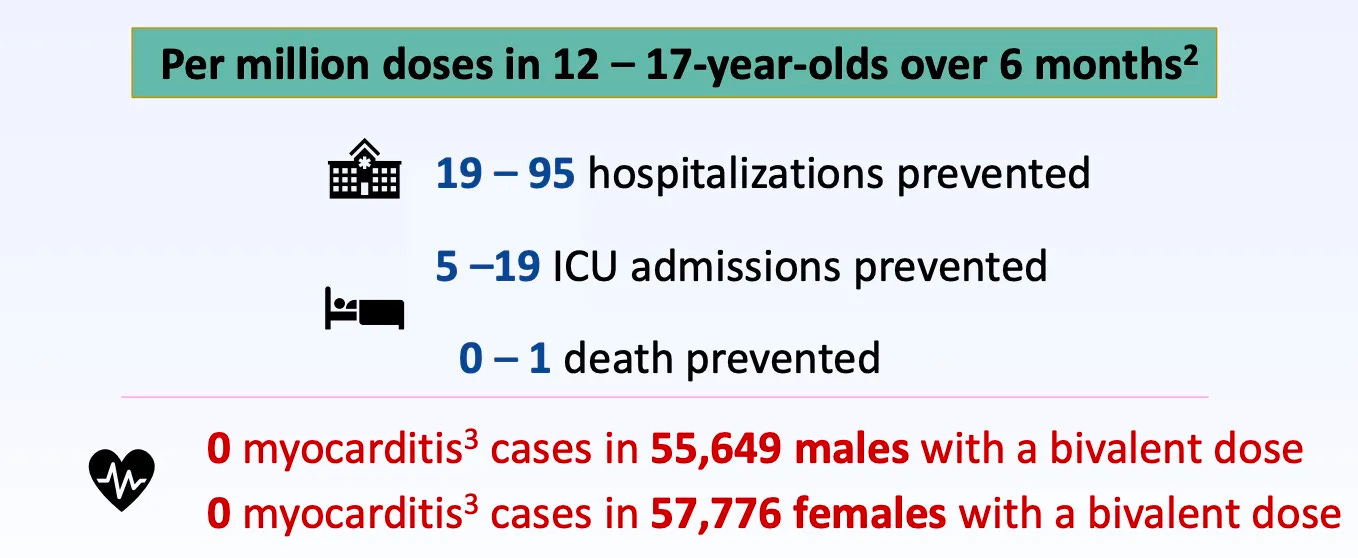
There was a true and rare safety signal for myocarditis among young males after mRNA vaccines. This has been under intense surveillance and was discussed in length at the latest FDA and CDC meeting.
But, after last fall’s updated Covid-19 vaccine, only 2 myocarditis cases were verified out of ~650,000 doses among young males and females. This is a much smaller rate than with the primary series. It’s about the same rate as background, which means it’s not a safety signal anymore. We think this is because the increased time interval between doses reduces risk. However, there is limited data, so this estimate has some uncertainty.
Although the risk/benefit ratio has changed over time, benefits continue to outweigh risks, even for adolescents.
Risk of clotting
Addressing his rumors is an entire post in itself, but here are a few important points that seem to cause repeated confusion:
The J&J vaccine was associated with a small increased risk of a rare kind of clotting disorder (TTS), not the mRNA vaccine.
Myocarditis does not mean an increased risk of heart damage from blood clots. Myocarditis is not caused by blood clots. These are separate processes.
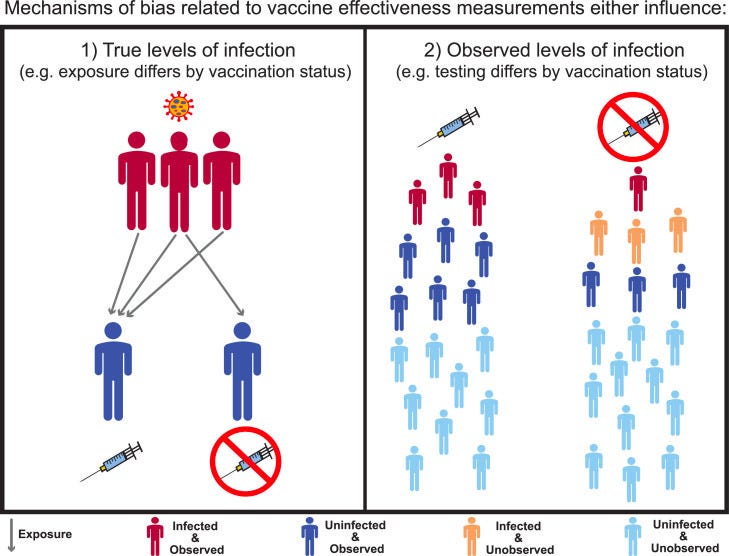
Negative effectiveness
Some real-world, observational studies show that vaccinated people are more likely to get infected after ~6 months compared to the unvaccinated. This is true.
There’s no immunological evidence to suggest the vaccines are actually harming immunity. So we are left with two hypotheses that have yet to be tested:
Bias. For example, vaccinated people may be more likely to be exposed more often (because they feel more protected). Or, those who get vaccinated are more likely to test (and thus, more likely to detect infection).
Timing. Even just the timing of when people got vaccinated, when the latest COVID wave went around, and when you assess for vaccine effectiveness can create spurious results if you’re not careful.
Spike protein in blood for up to 6 months
He cites a lab study that found protein fragments of the vaccine spike. This does not mean that the spike protein was circulating in these samples. The immune system processes proteins into fragments naturally, so finding a fragment doesn’t tell you that the spike protein is still intact or being produced. It’s like finding the letter “a” in a document and saying that the document has the word “aardvark” in it.
16% higher risk of serious adverse events in mRNA vaccine recipients
A 2022 study led by UCLA and the University of Maryland was published in Vaccine that analyzed the clinical trial data using different definitions of adverse events. Vaccine is a leading journal in the field, but it is not perfect. This particular study is incredibly messy and should have never been published. For example:
16% is not statistically significant— in other words, 16% isn’t any different than 0% increased risk of adverse events after vaccination (risk ratio=1.16; 95 % CI 0.97 to 1.39).
Authors compared number of adverse events, not the number of patients who suffered. This automatically skews the data because one person often has multiple symptoms (e.g., abdominal pain often accompanies diarrhea.)
Left out
There are important points completely left out of his argument, which shadow the larger picture too:
The impact of actually getting infected. The virus continues to be more concerning than the potential for vaccine side effects. The most recent example is an increased risk of cardiovascular disease and stroke due to artery plaque after Covid-19 infections.
We have other options. His biggest concern seems to be mRNA vaccine biotechnology. We do have another fantastic option that is not mentioned— Novavax—that uses a more traditional vaccine platform.
Muddling >65 vs. <65 debate. At this point, there’s a legitimate debate about whether vaccines should be approved for everyone or only high-risk. Country-to-country comparisons, for example, have bubbled up. However, lumping everyone together, as this narrative has, is neither conducive to nor helpful in reaching the most at-risk.
Common ground
It’s important to acknowledge there are points we agree on:
Medication (i.e., Paxlovid) is an important tool.
FDA should push for more evidence. This has been a loud theme from VRBPAC—the external committee to the FDA—throughout the pandemic. Why aren’t we getting T cell data? Why aren’t we getting B cell data? Why can’t we find correlates of protection for antibodies? We should demand data from pharma companies.
We should always work towards better vaccines. Thanks to the $5 billion Operation Next Gen we are developing next-generation vaccines that prevent transmission (like nasal vaccines) or are variant-proof (like pan-coronavirus vaccines).
Bottom line
Framing public health as anti-human is an incredibly dangerous game to play.
Health policy decisions need to be grounded in an accumulation of evidence that provides a comprehensive picture of reality. He combines legitimate points with profoundly foolish ones, which muddles the picture, creates a sense of false equivalency, and makes it difficult for the general public to discern the truth.
Keep this in mind when decision-making about Covid-19 vaccines this fall.
Love, YLE and KP
A big thanks to Edward Nirenberg for helping with the immunology points above.
Kristen Panthagani, MD, PhD is an emergency medicine physician at Yale. In her free time, she is the creator of the medical blog You Can Know Things. You can subscribe to her newsletter here.
“Your Local Epidemiologist (YLE)” is written by Dr. Katelyn Jetelina, M.P.H. Ph.D.—an epidemiologist, wife, and mom of two little girls. During the day, she is a senior scientific consultant to several organizations. At night, she writes this newsletter. Her main goal is to “translate” the ever-evolving public health world so that people will be well-equipped to make evidence-based decisions. This newsletter is free, thanks to the generous support of fellow YLE community members. To support this effort, subscribe below:
 | A guest post by
|
In a state with an incredibly old population, his advice really is public health malpractice. Fortunately, lots of folks here in Florida are moving ahead with vaccines, when they can find them.
Agreed. Benefits outweigh risks. Long term effects of illness are much scarier than a few spike proteins floating around. I fear coronary artery invasion, central and autonomic nervous system invasion, and post Covid conditions. I’m “pro-human” and therefore I’m getting my XBB booster today, and so is my daughter. I expect it will reduce my chances of getting infected for a while, and every time I don’t contract Covid is a pair of dice left uncast. I expect it will help reduce long Covid and collateral damage like previous vaccinations when I do get infected.
I’m not worried about hospitalization and death for my age group. But there is a lot of badness along a continuum that ends in death, and bolstering my defenses like an annual flu shot is what I’m talking about.
I’m very grateful, really.