



Measles, ACIP, flu campaign, bird flu, and telehealth ending
The Dose (February 24)

Happy Monday! A lot is going on in the world of public health. Here’s some health news you can use to start your week.
Your national disease report: Flu, flu, go away
There are a ton of sick people out there, but we are finally getting a reprieve. The number of people with “influenza-like illnesses” (defined as a fever, cough, or sore throat) took a dive this past week.
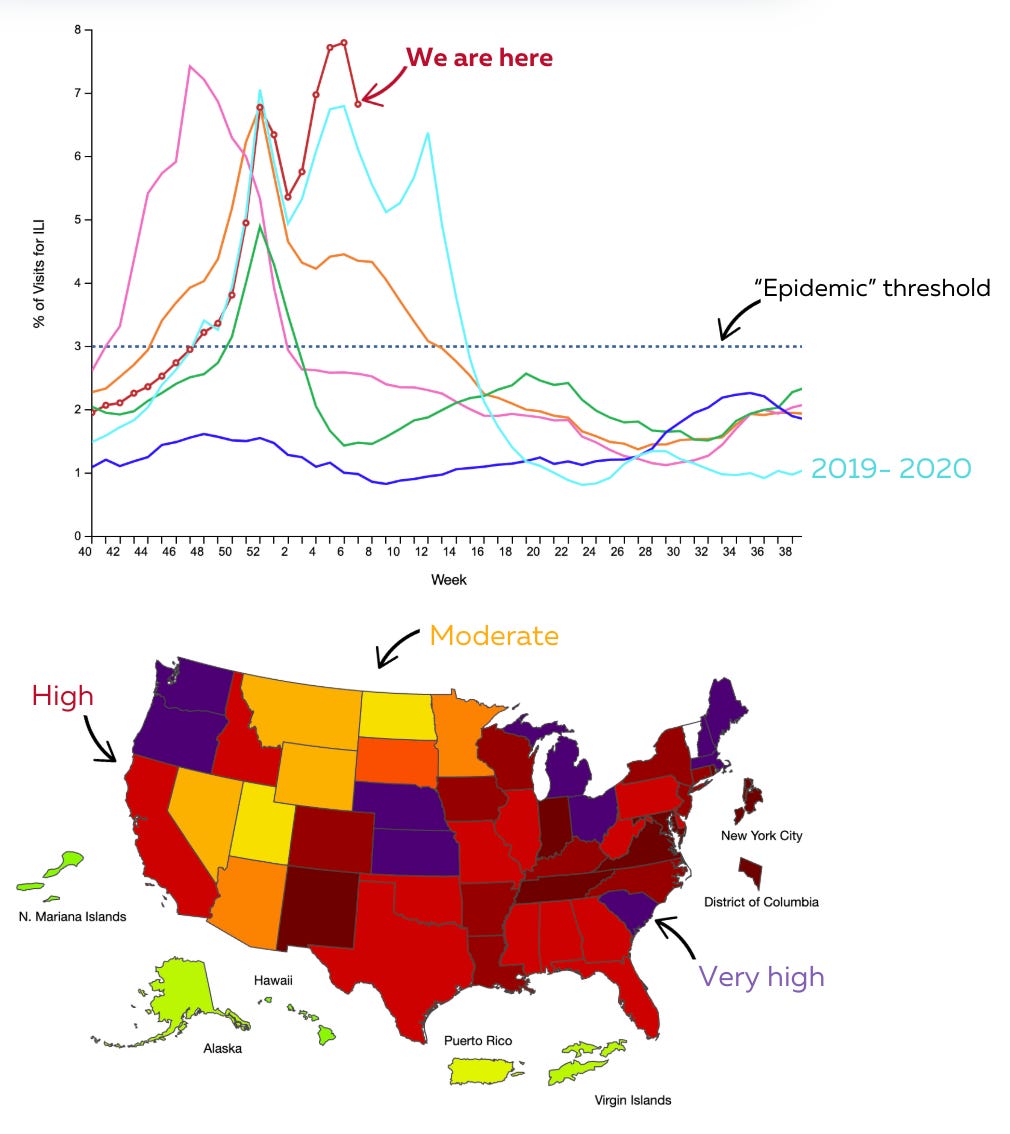
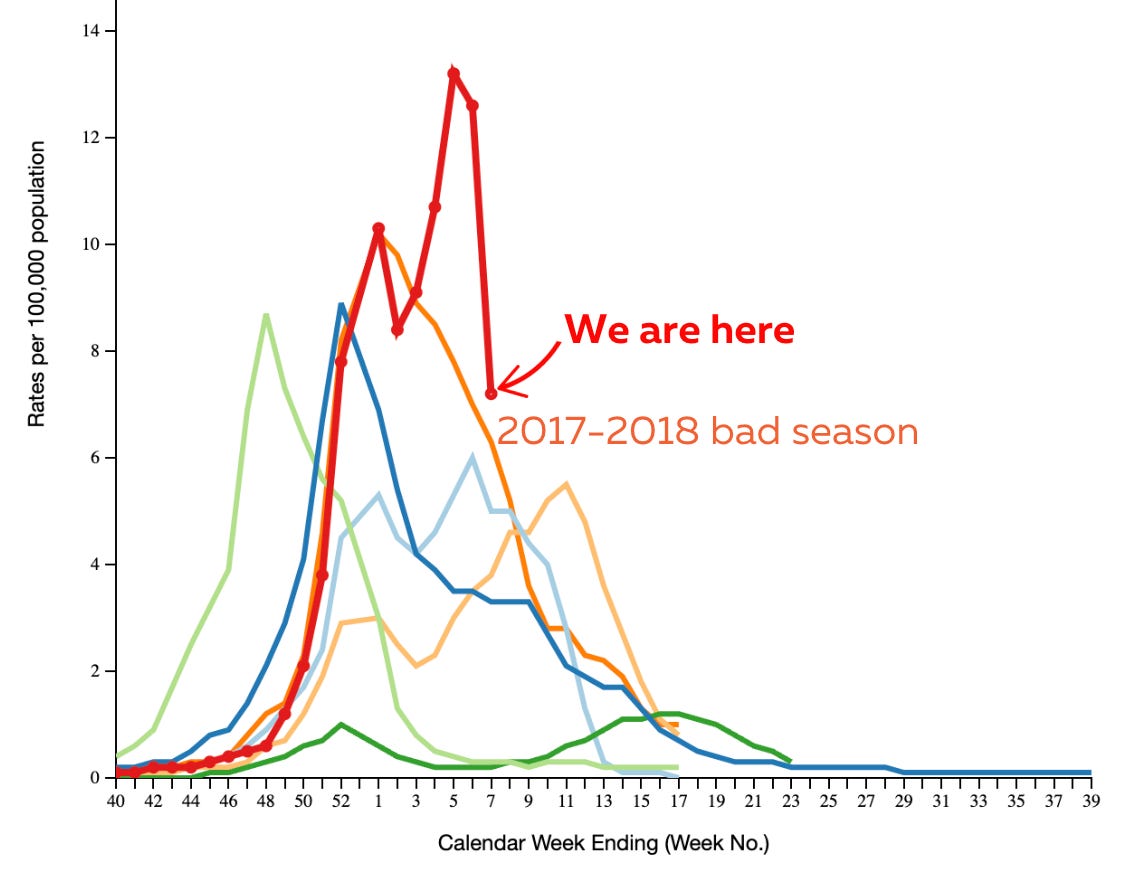
Flu is the main culprit and follows similar patterns—it’s high but has started retreating. Regardless, flu hospitalizations this year have already surpassed the last “very bad” flu season in 2017-2018.
It seems like a bad time to stop a flu vaccine campaign. Alas, the new HHS administration is discontinuing the “Wild to Mild” flu campaign on Wednesday. CDC has been using images to emphasize how vaccination can help control flu symptoms, which I appreciate because they better reflect the purpose of vaccines (avoid severe disease, not prevent infection).

RFK Jr. wants a campaign focused on “informed consent.” Informed consent is always important, and the flu vaccine can have a very rare safety signal depending on the season. But the benefits greatly outweigh the risks. Conflating the two could significantly impact uptake.
What does this mean to you? It’s not too late to get your flu shot. The flu season is notorious for having a long tail.
Measles is coming in hot
All eyes are on a Texas outbreak that is out of control. Here’s the breakdown:
Cases have risen to 90, with 16 hospitalized. The vast majority of cases are unvaccinated and school-aged.
This outbreak started in a tightly knit, unvaccinated pocket—specifically, a Mennonite community—but has now spread to five counties.
This region has a low vaccination rate—one in five students is not vaccinated for measles, mumps, or rubella (MMR).
How bad is this going to get? No one knows. But, as a fantastic epidemiologist pointed out, an increase of 32 cases in three days means the “force of infection” is strong. In other words, this is spreading exponentially, leading to more cases.
Another outbreak (9 cases) is growing in a neighboring county in New Mexico. An epidemiological link to the Texas outbreak hasn’t been made yet, so this may be a coincidence (although it’s hard to imagine it is).
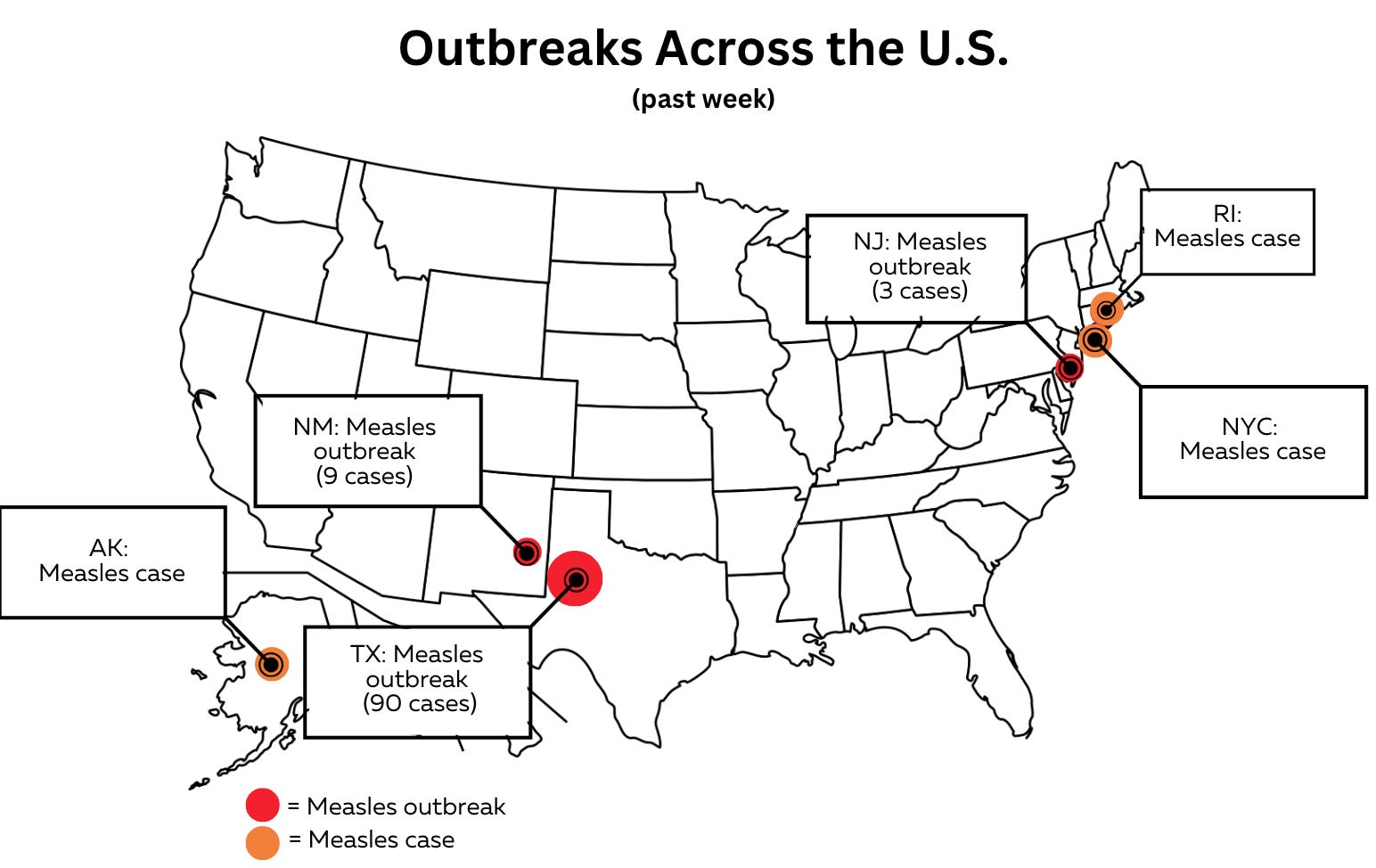
An outbreak in New Jersey (3 cases) is also being closely monitored, particularly because hospital exposure could accelerate the spread.
How quickly each of these gets under control greatly depends on the state and local health departments’ ability to respond quickly and effectively. This relies on the public’s willingness to cooperate in case interviews, people’s willingness to get vaccinated, and available resources and support.
What does all this mean to you?
If you are in an area with an outbreak:
Pay attention to local public health department communication, including areas where cases have been to avoid measles exposures.
If you have a child under 12 months old, they can get a vaccine early (at 6 months). Talk to your pediatrician.
If you’re up to date with vaccines, you are very well protected (although the vaccines are not perfect).
If you’re not in a hot zone:
Reconsider travel to West Texas, especially if you have a baby under 12 months, because they have no protection against measles.
If you were born after 1957 and vaccinated before 1968, getting another dose is a good idea. You got an older vaccine that used an inactivated virus, which doesn’t work as well.
You can check your MMR titers (not all immune systems that get two doses of MMR get activated). This can be more expensive than just getting another vaccine, but if you do have low titers, it could help with insurance coverage.
ACIP vaccine meeting delayed: Lookout for two things
ACIP—the external CDC advisory committee for U.S. vaccine policy comprised of pediatricians, scientists, and parents—was scheduled to meet this week, as they do every February. However, HHS postponed this meeting to an undefined date to allow for public comment.
This is the first time ACIP has been delayed. While allowing sufficient time for public comment is required by law before this committee meets, HHS has had since Feb. 3 to open for public comment. And it’s still not open.
This may reflect a chaotic administration transition. Another possibility, which I think is more likely, is that RFK Jr. is buying time to restack the ACIP committee roster to include people more aligned with his warped vaccine views. Politico reported that RFK Jr. plans to replace members who he perceives to have conflicts of interest. This is curious: ACIP members already disclose their COIs publicly, which is designed to prevent COIs from influencing decisions. ACIP has long been the gold standard for open, transparent recommendations on vaccine safety and effectiveness.
I’m certain misleading and inaccurate information about current ACIP membership will be made. As this unfolds, look out for two common tactics used to promote falsehoods:
Context removal: Misleading narratives may frame these disclosures as evidence of corruption rather than a safeguard against it. A COI from 30 years ago is much different from a current COI. Blurring the line erodes trust.
Attack on expertise: The overlap between medical and scientific professionals and pro-vaccine positions is nearly universal—because vaccines work. But expect to see this expertise reframed as bias or even conspiracy, like: “Of course all these people support vaccines, they’re part of the same system!”—ignoring the fact that their support comes from overwhelming evidence, not collusion. Undermining trusted experts makes space for less qualified voices to shape policy and public perception, often to the detriment of public health.
What this means to you today: We won’t get updates on many things, like how the flu vaccine is holding up, how antibodies should be used to keep babies from dying from the RSV virus, which travelers should receive a new vaccine against Chikungunya (which causes very bad joint pain), and more. A lack of transparent, open, and honest information about vaccine safety means communities can’t make their own informed, data-driven choices.
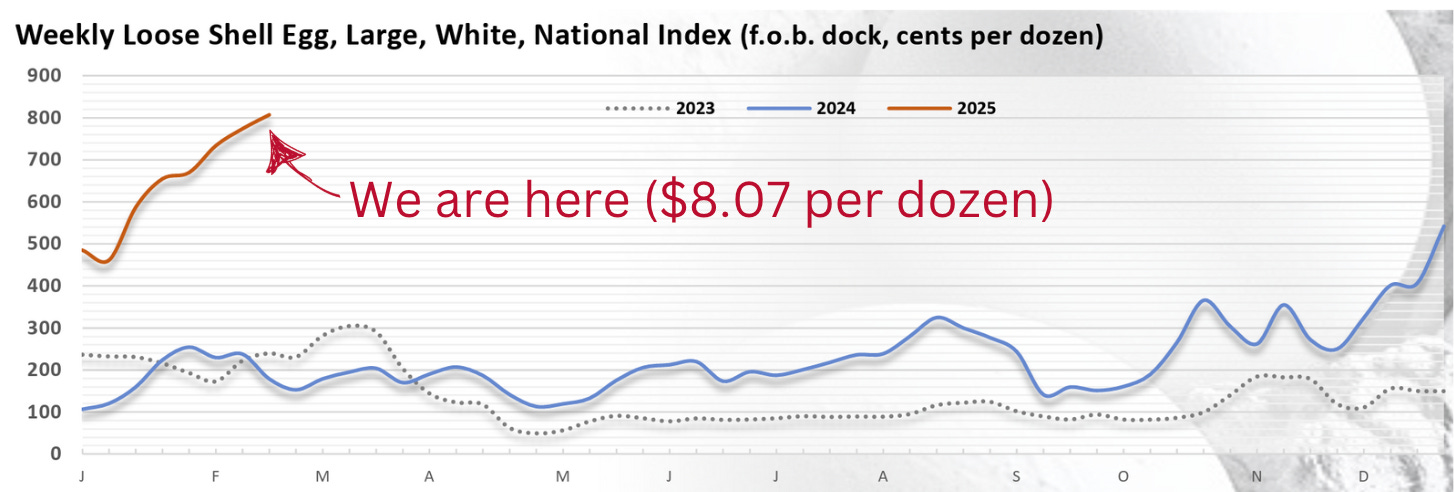
Bird flu (H5N1) and egg prices up
Egg prices continue to skyrocket due to the bird flu pandemic ravaging poultry farms. The average cost for a dozen eggs is now slightly over $8.00.
Given pressure, the new administration has suggested some policies, like vaccinating and medicating poultry and quarantining sick flocks. Like any policy, though, there are important considerations. I outlined them on PBS NewsHour last week:
A new publication from CDC (after being delayed for 4 weeks) found a transmission pathway (humans -> house cats). In these cases, cats were exposed to dairy workers with H5N1 symptoms. Cat-to-human transmission has also been documented in the past with avian influenza.
Should you worry about your cats? Farm cats are at high risk (drinking raw milk). Risk to house cats is very low on the list of things anyone should worry about at this point. But don’t serve your cats raw pet food. There have been a couple of outbreaks of cats now linked to raw pet food.
Heads up: Medicare will stop covering telehealth in April.
If you’re on Medicare and have leveraged convenient telehealth appointments, that’s about to end.
Medicare originally expanded its coverage of at-home telehealth services during the Covid-19 emergency, which was an important move to protect seniors and has become a critical service for those in rural communities.
As part of the deal to keep the government open in December, Congress proposed a bill to extend telehealth coverage for two years. However, Elon Musk struck down that bill; the ultimate package that kept the government open only extended coverage through March 31.
The change doesn’t apply to all telehealth services: for those in urban areas, monthly home dialysis visits for end-stage renal disease, acute stroke, and mental/behavioral health visits can still occur via telehealth. For those in rural areas, people must be at a healthcare facility to access telehealth services.
Poll:
Bottom line
You’re all caught up for the week! Stay healthy out there.
Love, YLE team
Your Local Epidemiologist (YLE) is a public health newsletter with one goal: to “translate” the ever-evolving public health science so that people feel well-equipped to make evidence-based decisions. This newsletter is free to everyone, thanks to the generous support of fellow YLE community members. To support the effort, subscribe or upgrade below:
Worry—about everything! We appreciate you keeping us informed in the midst of a government that opposes science and public health.
Do you foresee the CDC vaccine guidelines/scehdules being updated significantly under the current administration?How concerned should we be about vaccine access being impacted for those of us that want to continue to vaccinate ourselves and children (i.e., follow the CDC guidelines in place prior to the current administration)?