



Myocarditis, preprints, and the UK

There is a lot of discussion and misinformation circulating (again) regarding vaccine-induced myocarditis (i.e. inflammation of the heart) among adolescents. This is important to address because only 40% of 12-15 year olds are fully vaccinated and the remaining parents/adolescents need accurate, evidence-based information. We should also be proactive and prepare for questions from parents of 5-11 year olds as this vaccine is coming soon.
As far as I can tell, the myocarditis concerns have been re-fueled by two things:
A preprint released last week; and,
News that the UK Joint Committee on Vaccination and Immunization did not recommend the Pfizer vaccine for 12-15 year olds. (But today this decision was reversed).
As you can imagine this has made waves among the public (and particularly parents) trying to navigate this ever-stressful landscape. Here is the evidence-based breakdown…
Preprint
Last week a preprint was released that concluded Americans/CDC/FDA should reconsider vaccinating healthy adolescents because the risk of vaccine-induced myocarditis outweighs the benefits of vaccines. With discussion of this preprint, there is a lot of important context lost. Here are some important points you should consider…
Notice that this preprint leveraged VAERS data. We have to take VAERS with a grain of salt. While it’s very useful in finding safety signals and finding hypotheses, it’s a passive surveillance system. This means anyone can report a case here and it’s not verified. In multiple places on the VAERS website you can find warnings like: “The reports may contain information that is incomplete, inaccurate, coincidental, or unverifiable” or “The inclusion of events in VAERS data does not imply causality”. VAERS is not comprehensive and certainly not rigorous enough to make sweeping causal statements like the authors did.
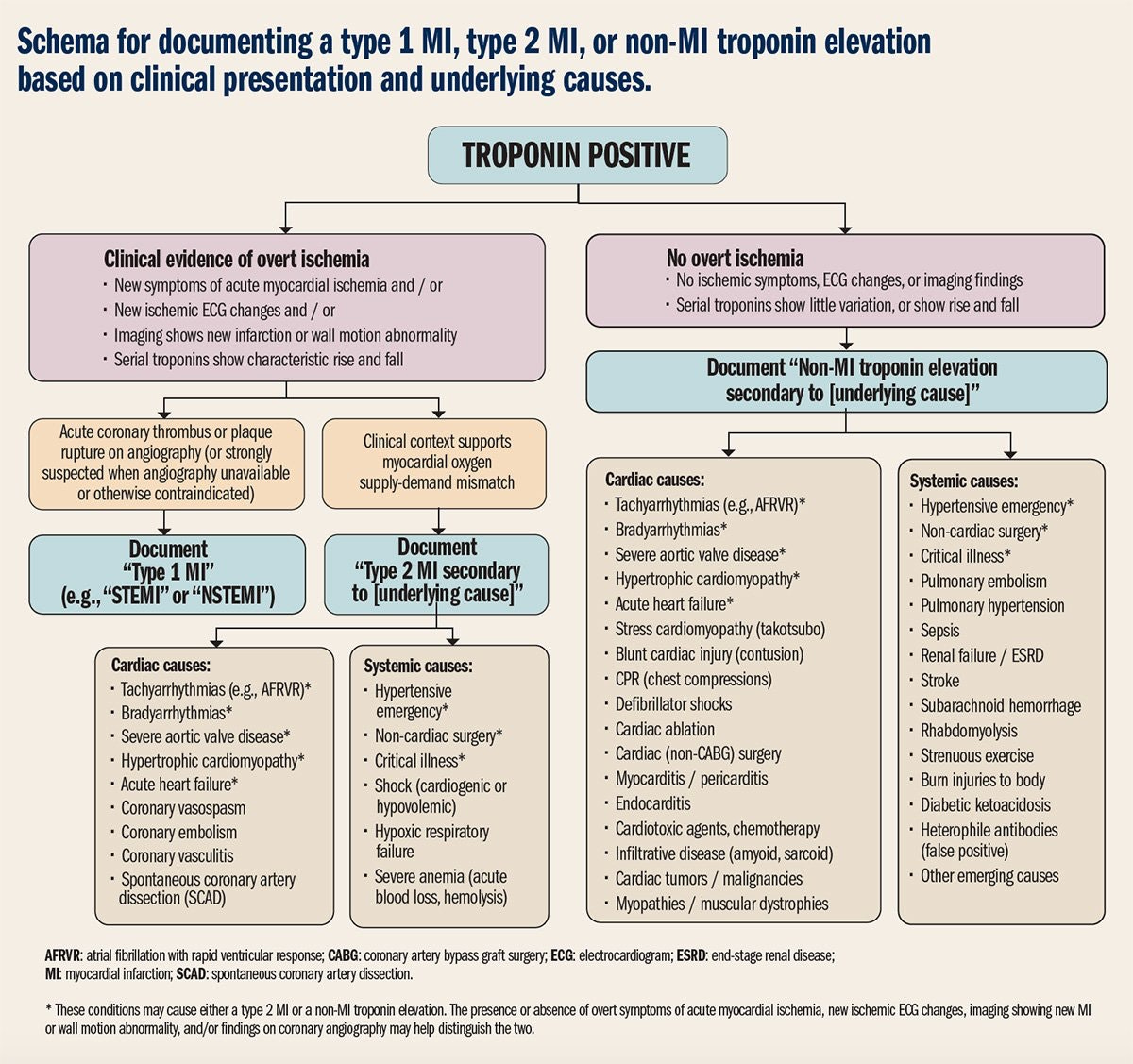
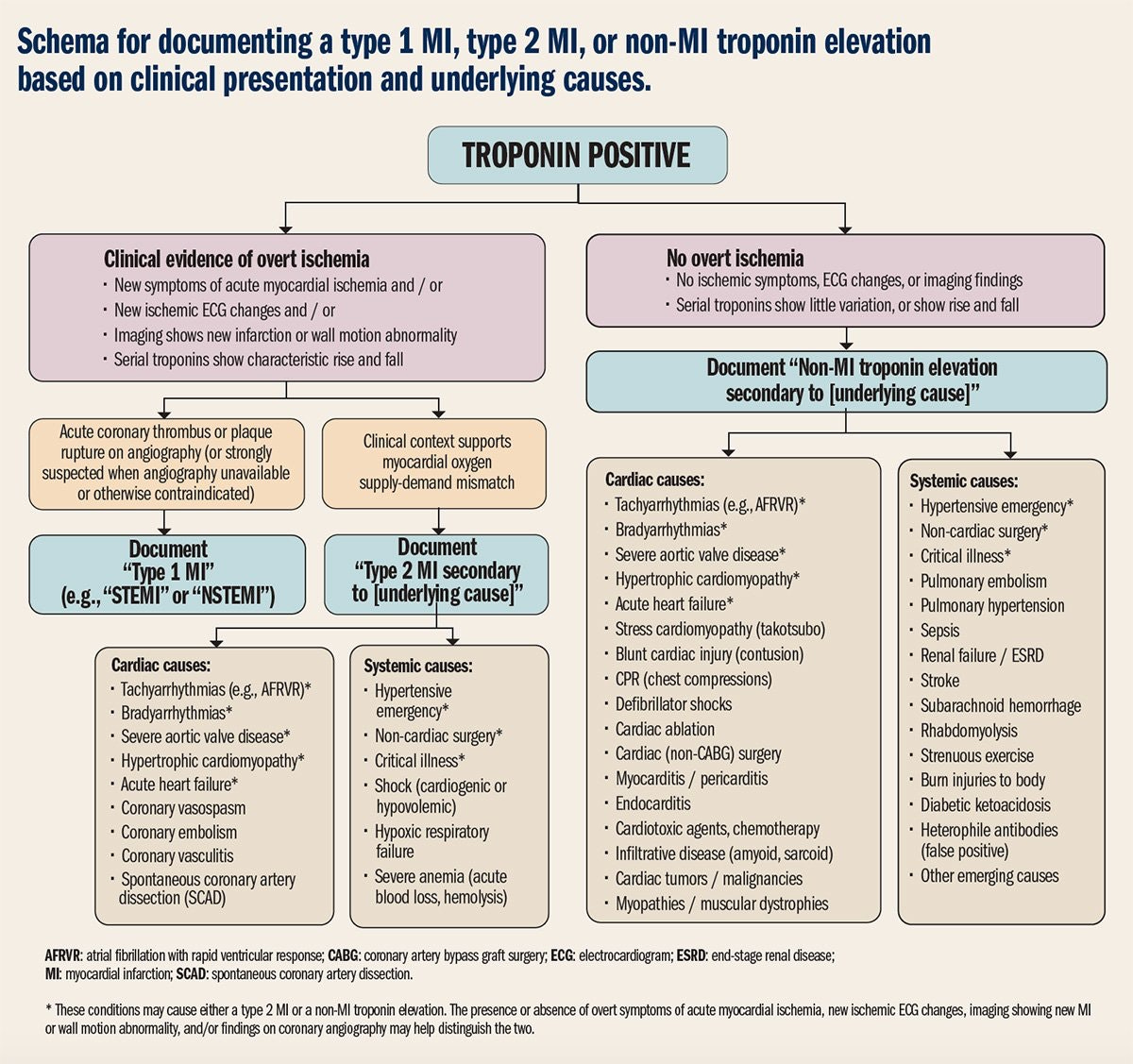
The authors did not have full, unlimited access to the raw VAERS data; they just used the publicly available data. Which you or I could also do by downloading it here. This is important to note because they weren’t able to investigate each one of these cases. Because they weren’t able to do this, they counted every case labeled “high troponin” (a heart protein) as “myocarditis”. But that’s just plain inaccurate. High troponin can mean a lot of things (see figure pulled from the American Academy of Cardiology below). For example, you release troponin from exercise. Each of these cases need to be thoroughly investigated to make a causal link. This is literally a cardiologist’s job and this preprint did not do this.
There is a spectrum of myocarditis severity. While it’s important not to minimize true myocarditis cases among vaccinated, it’s important to keep a healthy perspective. Myocarditis among boys after vaccination is mild. And, in a new study in the journal of Pediatrics, people with myocarditis after vaccination fully recovered: “The hospital course is mild with quick clinical recovery and excellent short-term outcomes”.
Finally, notice the list of authors from the preprint. Recognize them? If not, you can find my critique of their latest Op Ed here.
UK Policy Decision
The other thing fueling the myocarditis discussion is a recent UK policy debate. On Sept 3, the UK Joint Committee on Vaccination and Immunization (JCVI) conducted a risk-benefit analysis on myocarditis and vaccination of 12-15 year olds in the UK. They made a newsworthy decision to not recommend vaccinating healthy 12-15 year olds. Children aged 12-15 years who are vulnerable to COVID-19 or who live with an at-risk person were eligible.
They made this decision based on a rough estimate that the rate of pediatric ICU admission for children aged 12 to 15 years without underlying health conditions was 2 per million. This is compared to a rate of over 100 per million for those with underlying health conditions. The reported the risk of myocarditis in the UK is 3 to 17 per million for the first dose; and 12 to 34 per million for the second dose.
Some have agreed with this decision, saying it’s a marginal benefit and focused on the health of vaccine recipients. But many scientists and clinicians disagreed with their assessment saying the analysis was very, very sparse. JCVI shockingly published little information of their risk-benefit analysis given the massive implications. The analysis also underestimated the risk to children of severe disease, which then of course underestimates the benefits. The assessment didn’t consider myocarditis impact from COVID19 disease. They didn’t take into account kids’ integral role in SARS-CoV-2 transmission and did not take into account long COVID-19.
But JCVI was just a recommendation. The final decision laid in the hands of UK’s chief medical officers who said today: Universal vaccination of one dose for 12 to 15 year olds.
For parents that want the full U.S. context…
On May 23 (1 month after EUA for adolescents) the CDC/FDA found a safety signal in the adolescent surveillance data: vaccines may cause mild and temporary inflammation of the heart. On June 23, the CDC met to review all of the data and conduct an extensive risk/benefit decision (here are the cliff notes). They concluded two things:
There was a causal link between mild myocarditis after vaccination, especially among young boys;
The benefits greatly outweighed the risks.
After this meeting, further research found that this is happening because the mRNA vaccine triggers the immune system which then temporarily inflames the heart. This is why myocarditis is more common for the second dose compared to the first dose.
Since then, we have had an overabundance of published scientific studies that confirm benefits over risk:
The ACIP (external committee for CDC) continues to monitor the data and continually reassess benefit/risk ratio in the United States. The latest update was on August 30. This update was also based on VAERS, but the key difference is that the CDC has access to the raw data AND investigates each case in depth through interviews with patients and consultations with cardiologists. During this meeting, ACIP confirmed that the benefits of vaccination still outweighed the risks of mild myocarditis.
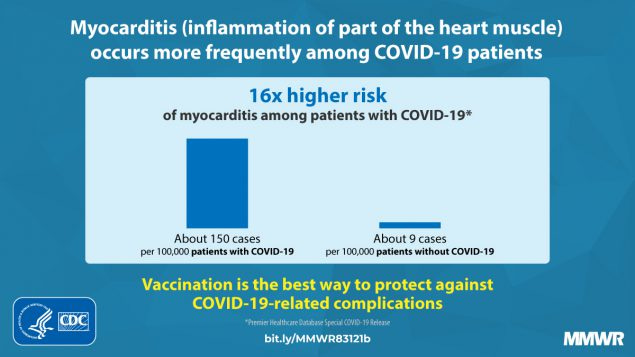
Importantly, many studies have also found substantial risk of myocarditis with COVID19 disease. In this study, which looked at multiple medical events, risk of myocarditis among unvaccinated was much higher than among vaccinated. In this study, the risk of myocarditis was 16x higher among COVID19 disease than people without COVID19. Here is a peer-reviewed article describing myocarditis among 20 kids with COVID19 disease, which led to MIS-C.
Bottom Line: This is such a hard time for parents to navigate, but please consider the broader context when preprints are circulated or decisions are made overseas. In the United States, it’s strongly recommended that anyone 12+ years get vaccinated right away. The benefits continue to greatly outweigh the risks.
Love, YLE
P.S. Thanks to Dr. Jenn Dodd, a friend and brilliant epidemiologist at Oxford, that helped me parse through the UK situation for a balanced approach.
I also feel need to point out that the preprint authors are largely in sports medicine, NOT cardiology.
Once again, I'm horrified by the mis-use of preprint writings!
I even hesitated to report a serious Moderna reaction of my young adult daughter to VAERS,
Because the data is not verified in any manner.
She already has unspecified autoimmune dysautonomia, but she desperately wanted vaccination.
We made sure to report her pre-existing conditions so that it was not mis-interpreted.